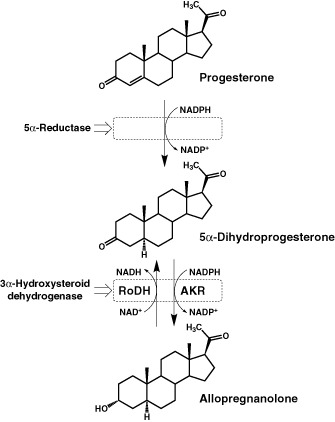
I’ve also included an image showing the metabolic pathway from progesterone to allopregnanalone. As you can see, the same enzyme that converts 3α-androstanediol to 3α-diol-G also converts progesterone metabolite 5α-dihydroprogsterone into allopregnanalone.
Guys, I think this really might be the enzyme we need to zero in on. It covers everything - both the sexual and the mental symptoms, AND accounts for the consistently low 3α-diol-G that so many of us see in our lab results.
Short term user here as well (6-7 days with immediate crash right after – fuck us, right? haha). Your thought process seems sound; I hope this works for you. Please keep us updated and good luck.
Burt, thank you very much for creating this thread. Have you had your levels for 3a-diol-g and Allopregnanolone tested? After reading the stop the thyroid madness II book I have a much more open view on the probably of the gut being involved than I did before. Anyway, I’m so glad the studies are finally narrowing in on things the way the finally are. Looking forward to seeing your follow ups.
What is Ethynylandrostanediol and who has been shown to be low in it? or what studies have shown PFS groups to be low in this? I have never heard of it and want to know more about this metabolite…
Do you know the name of the drug that was in development 5-10 years ago that was an analog to 3a-diol-g?
It makes sense that if 3α-hydroxysteroid dehydrogenase was inhibited that our 3a-diol levels would be low. The thing with 3a-diol though is that the two PFS neurosteriod studies that I am aware of DO NOT show 3a-diol levels to be low. It’s not low
in the studies or in the three of us that had ours tested. Starting with the results from the three of us on this website that had our levels tested in 2013:
Scaredoutofmymind’s results:
3b-Adiol was 13.1 (on a range from 4.0 - 20.2)
3a-Adiol readings where 6.4 (On a range from 2.3-10.5).
His 3a-Adiol readings are clearly not low.
Spstriken’s results:
3b-Adiol was 7.0 (on a range from 4.0 - 20.2)
3a-Adiol was 4.0 (on a range from 2.3 - 10.5)
His 3a-Adiol readings are a little lower than Scaredoutofmymind but are clearly not low and are pretty much almost in the middle.
My 3b-Adiol was 3.7 (on a range from 4.0-20.2)
My 3a-Adiol was 3.3 (on a range from 2.3-10.5)
My 3b-Adiol readings are flagged as low but my 3a-Adiol are not, however they are on the lowish end of this labs range. So for me personally there could be something going on with 3a-Adiol and deff 3b-Adiol but I’m still only one out of the three of us showing this. To further illustrate my point lets compare the 3a-diol readings from the PFS groups from both PFS altered neurosteriod studies:
The 3a-diol findings in the “Neuroactive steroid levels and psychiatric and andrological features in post-finasteride patients” study were found to be increased in the CSF of the PFS group and uneffected in plasma of the PFS group.
The 3a-diol findings in the “Patients treated for male pattern hair with finasteride show, after discontinuation of the drug, altered levels of neuroactive steroids incerebrospinal fluid and plasma” study were found to be increased in the CSF of the PFS group and increased in plasma of the PFS group.
So both PFS neurosteriod studies from 2013 and 2014 did not find 3a-diol to be low nor was it low in the three of us who had ours tested. Instead both studies found 3a-diol to be increased in CSF of PFS patients and one of them found 3a-diol to be high in plasma while the other one found 3a-diol levels to be uneffected in plasma.
Are you aware of any PFS people that have low 3a-diol readings ? According to the studies low 3a-diol readings are not the norm for PFS people.
Do you have any good studies on DHT inhibitors inhibiting 3α-hydroxysteroid dehydrogenase? You posted what 3α-hydroxysteroid dehydrogenase does but not anything specific about DHT inhbitors inhibiting this enzyme. I have read somewhere before that finasteride and dutasteride also inhibits 3α-hydroxysteroid dehydrogenase but I forgot about this and cannot recall the source. Do you have any that you can post? This is kind of a big oversight seeing that no one really ever consideres the implications of inhibiting this enzyme and the focus is always on 5Ar
Trying to upregule 3a-hydroxysteroid dehydrogenase would seem logical just like we are always trying to increase 5ar. Replacing Alleopregnanlone has more or less been done already in a handful of us over on the ray peat forum and swolesource. Except that we did not have access to Alleopregnanlone directly. We took 5aDHP which converts to Alleopregnanlone. If I remember correctly Prog converts to 5aDHP via 5AR and that 5aDHP converts to Allopreg using a different enzyme that I can’t remember. The majority of us that tried 5aDHP got at least some improvements, some more than others. I personally got the best results from 5aDHP that I have seen from anything else I tried. I don’t have blood work to prove it but there is no doubt in my mind that I am low in 5adhp and Allopreg. However increasing Allopreg by increasing 5aDHP was not a silver bullet and was not a cure.
I agree that taking progesterone would cause a slight increase in Allopreg. You would get a much better increase in Allopreg by taking 5adhp though. I also agree that the fact that most men with this condition having normal DHT and T levels tells us that if altered hormones are to blame that its 5ar reduced metabolites further down the pathway
As far as upregulating 3α-hydroxysteroid dehydrogenase goes using Progesterone cream, Do you have any studies or sources that shows that this is possible? Obviously I would first want to see conformation that DHT inhibitors inhibit 3α-hydroxysteroid dehydrogenase in the first place but upon confirming this the next thing to do would be to start researching how to increase it.
“Various antidepressants, including theSSRIs fluoxetine, fluvoxamine, sertraline, and paroxetine, the SNRI venlafaxine, and mirtazapine, have been found to activate certain 3α-HSD enzymes, resulting in a selective facilitation of 5α-dihydroprogesterone conversion into allopregnanolone”.
I agree that doctors and even the scientists at MERK do not completely understand whether
pro-sexual effects men feel are from DHT metabolites or T/DHT themselves and that T and DHT may not be able to induce their intended androgenic effects with out being converted into their end metabolites.
Altered neurosteriods seem to be the most logical thing to investigate as of right now. Hopefully more studies will look into this and try to find patterns of altered neurosteriods that all or most PFS people have.
You bring up important points, especially with regard to ScaredOutOfMyMind’s results. I’ve been thinking about this a bit more and I’ve come to a new conclusion, based on other lab results of men before and after finasteride and my own personal history.
I think post-finasteride syndrome is primarily a disease of the endocrine system, first, being completely unstable and trying to find an equilibrium, and then that new equilibirum being found but then being inadequate/far less enjoyable than the pre-fin equilibirum.
There’s clearly a difference between men who took fin for years and men who only took it for a short period of time and then crashed. And of course most men who take fin have an endocrine system that knows how to get back to the way it was before fin and stay there. We, for whatever reason, have systems that either refuse to go back to the way things were or have lost the knowledge of getting back there altogether. Either our systems can’t handle to workload necessary to establish a pre-fin equilibrium, or an epigenetic change occurred that obscured that blueprint.
I think we’ve established a new balance. The fact that I’m losing my hair just as much as I was pre-fin and that my semen is viscous again suggests that my 5-ar-2 enzymes are functional, and it probably also suggests that my enzymes downstream from there are likely functional. The fact that, while I was crashing, there were certain days/weeks when my libido was back to the way it was before fin shows that the issue is not neurological (except in very severe cases, usually involving guys who took the drug for years) or vascular, as those changes tend to be permanent and do not fluctuate outside of an autoimmune disease like MS (and there’s very little evidence to suggest that this is an automimmune disease).
I believe that during our initial crash and the period immediately after our systems have just been shattered and they’re scrambling to pick up the pieces. It doesn’t know what normal is so it tries to determine that. This results in chronically changing hormone levels system-wide. There are men who, in their crash phase, have hormone levels that fluctuate enormously (one guy had T values in the range of 90-1200!). The best thing to do during this phase is to manage mental and sleep symptoms as much as possible, but to try and not perturb hormones too much. I took a lot of ativan during this time, although I made sure to never take any for more than 3 days in a row, due to the risk of very nasty withdrawal. Melatonin and 5-HTP are good ones as well. After a period of time our systems become stable, but it isn’t what it was before fin. Once the system becomes stable it doesn’t even try to improve anymore because it is well aware of what happens when it does try to change things. At this point, it’s best to get a broad hormone panel to see if anything is out of range, even slightly, and address whatever is.
Of course, ideally we would all have had hormone profiles before using fin, but for the vast majority of us this isn’t the case, and this is the main issue. I think if we knew what our T/DHT/E/prolactin/thyroid/cortisol/etc levels were before we started using this drug, we’d be able to attack our issues far more effectively. We would see how the numbers have changed. Because even hormones within the normal lab result range may not be normal for a specific patient, i.e. a man who had a prolactin level of 3 ng/mL and T level of 600 ng/mL before fin may not function with 7 ng/mL of prolactin and 400 ng/mL of testosterone, despite those being within range for the male population as a whole.
And this explains why T replacement therapy doesn’t work on many men, but it does work for some, and why anti-estrogen therapy makes some men better but others worse. Everyone here has established a new equilibrium and what works for one man will not necessarily work for another. Now, that being said, it does appear that addressing DHT and E will yield better results in men who took finasteride for a long period of time (>6 months). I think what the long-term sufferers are affected by the most is their endocrine system establishing a new balance WHILE ON THE DRUG. Some of them still crash, of course, but a lot of them are more likely to just remain the way they are even after coming off of fin. For the rest of us, nothing is going to help until our systems recover from the crash phase, which is going to vary. For me, I only took fin for 8 days and it took my body 2 months to find some level of stability and 6 more months to move on from crashing altogether. During the first two months I went through periods of extreme anxiety, horrible sleep, anhedonia, complete impotence followed by periods of normal sexual desire, good sleep, normal emotions, etc and that process cycled. The next 6 months exhibited these fluctuations to a much less severe degree. By 8 months in I could tolerate vigorous exercise and my crashes were gone, but I don’t have the sex drive I used to. This has been the main problem post-crash phase for me.
Fortunately, I did get my thyroid and T and E levels checked before taking finasteride, because I knew of the horror stories. Sadly, I never thought I’d end up as one of the victims of PFS, because I thought the illness only happened in men who take the drug for long periods of time and ignore their symptoms when they appear. How wrong I was. I intend to see an endocrinologist soon to have all of my hormones checked. I suspect, due to my lower sex drive, that prolactin is going to be either above range or at the very high end. This tends to be very common in PFS victims, and I’d wager that it’s the primary cause of most of our lowered sex drives. If my suspicions are accurate, then I’m going to try to get a cabergoline prescription. Many mmen have reported significant imporvements taking this. One man even said that it got his sex drive to where it was pre-fin. Other men swear on yohimbine as well, which I believe also lowers prolactin, albeit to a less significant degree.
I’ll let you know what the results yield and how they compare to my pre-fin labs, and how cabergoline or yohimbine work.
Update: Tried yohimbine last week with very disappointing results. Strangely enough, not only did it fail to deliver any sexual improvements, but I didn’t feel much of anything at all on it. No elevated heart-rate, no increase in energy levels, nothing. Maybe I’m just one of the people who doesn’t respond to it.
At the moment, because my primary care doctor fails to recognize this as a real condition, I’m forced to wait until December before seeing an endocrinologist and get a proper hormone panel. In the meantime, I’ve been looking into substances that may increase 5 alpha reductase activity and HGH secretion. I’ve been taking creatine, glutamine, and GABA for the past few days. Remarkably, on August 24th I noticed that my libido, for the first time, resembled my pre-finasteride libido. This was unbelievable to me and showed me that I likely don’t suffer from permanent damage. Sadly, it was gone by the next day. However, given that it increased in tandem with taking these supplements combined with lifting the night before, it suggests that there may be something to the idea of chronically lowered 5AR2 and 3a-HSD activity after all, especially combined with the chronically lowered 3a-diol-g levels seen in nearly all PFS patients (other than ScaredOutOfMyMind - that one’s an outlier).
I’ve ordered phosphitidylcholine and Butea Superba Extract, both of which have been witnessed to dramatically increase 5AR2 activity. I believe Moonman even spoke of a several month long remission while on a phosphitidyl complex (unsure whether it was -choline or -serine, but my research shows that choline may be more effective anyway). I’ll try p-choline as soon as I get it. I hope that it, given Moonman’s history with it, this finally pushes me out of this bullshit when combined with the HGH-increasing supplements I’m currently taking. I will keep you all updated. If this doesn’t work, I will move on to p-serine. If that fails, then cabergoline may be my last hope, and of course only if I have elevated prolactin to begin with. Then again, there is always the Baylor study, which is supposed to be published this Fall. I think we’re all really looking forward to those findings.
Sorry to come to this topic so late…
Remembering that finasteride was also a chem used in the treatment of prostate cancer/enlargement , I noticed that 3alpha hydroxysteroid D has a role in lethal castration resistant prostate cancer (CRPC) a third pathway to intertumeral synthesis of DHT.
It would seem in trying to reverse/upregulate the availability of this 3alpha we could be precipitating an undesirable process/outcome within the prostate!
Damn I totally forgot about this thread. Pretty much everything I tried in 2017 failed to do anything. I used peptides in 2018 (like BPC-157 and TB-500). BPC caused noticeable improvements in orgasm and affect but I’m pretty sure that was due to its indirect effect on dopamine. Semax helped a little cognitively. I still had watery ejaculate, sleep problems, and some anhedonia so its clear BPC didn’t address the core problem. All of these improvements failed to stick. None of the other peptides that I tried (Epitalon, TB, IGF, Melanotan II, PT-141) did anything.
Early this year I tried a month of saw palmetto extract and topical SP, which improved my sleep from about 4.5 hours at a time to averaging 6 hours, and improved my affect and libido quite a bit (still had orgasm issues and watery ejaculate though). So far I can say that directly antagonizing 5AR has helped me the most. I will probably cycle Fin at some point, but only because I’m assuming everything else is going to fail. I recognize the risks with using Fin again, even for only a few days, so don’t bother convincing me not to do it. I don’t consider this condition worth living with, and if I’m going to die anyway then I might as well throw everything and the kitchen sink at it.
As far as 3a-hydroxysteroid is concerned? I have no idea anymore. It is clear that our 3a-diol-g is low though, so I still think the problem is less from 5AR and more from things downstream of it. I think this finding is shared by people with Post-Accutane Syndrome.
5ar and 3a-HSD are mutual antagonists and both are needed to create ALLO which would improve sleep.
If your 5ar was too high, it would make your 3a-HSD too low and then you cannot produce ALLO.
That’s my theory for myself as my DHT levels are normal, which may mean normal 5ar but low 3a-HSD.
I’ll try to boost both together, 3a-HSD using sulforaphane and Glycine, and 5ar using creatine and Tribulus Terrestris. Of course, I’ll try boosting 3a-HSD first and will boost 5ar only if sleeps gets better and sexual symptoms worst.
Your sleep improvement using saw palmetto only encourages me to try and find something that boosts 3a-HSD without touching 5ar (other than by antagonizing it with 3a-HSD). Saw palmetto is a 5ar antagonist as we all know. It’s akin to fin and dunasteride. One effect inhibiting 5ar would do is to increase 3a-HSD.
It also shows it’s not your body’s blueprint that has changed, but only your hormone balance which has stabilized in an uncomfortable way.
I think @Burt_Kocain is right with his assessment that after the crash, there’s a fluctuation period and the first thing to address is to stabilize the body. I did this with a ketogenic / carnivore diet with lots of protein, saturated fat, and no carbs. I pretty soon added no carbs protein shake and when I stabilized, added some aminos like 5-HTP, Tyrosine and L-Dopa.
Now I’m stable, with insomnia well in-bedded in me. I will try Sulforaphane as it has shown to increase 3a-HSD without touching 5ar. It’s a broccoli sprout extract as I’m not too fond of drugs.
@Burt_Kocain, you’re on a suicidal path. Just give me a few weeks and I’ll come up with results from boosting 3-a-HSD and lowering 5ar. I’ve written a regimen that, for me, eliminated all symptoms except insomnia. Brain fog, anhedonia, anxiety were the first to go.
Try some of those below, you can always try saw palmetto and finasteride later if you really must. (And I think you shouldn’t, it’s been done before: people get better, than worst and stay worst, but as you say it’s useless to try and change your mind)
Well, I don’t intend on trying Fin again for at least a month anyway. I thought I’d try a 2 week water fast and a month-long NoFap period just to see if they help at all. If you get positive results then of course I’ll try sulforaphane instead.
EDIT: I cancelled my previous order of sulforaphane capsules in favor of buying broccoli sprouts, as there’s no evidence of bioavailable sulforaphane in capsule or pill form that I’ve seen. Apparently an enzyme called myrosinase that’s required to convert glucoraphanan into sulforaphane, which is released only by chewing the actual sprout.
I also came across a study comparing the levels of DHT in people eating alfalfa vs broccoli sprouts, and comparing both to baseline.
While the final results suggested broccoli sprouts didn’t significantly lower DHT, in the Discussion section the authors state "… we could not exclude the influence of alcohol. Based on our hypothesis, SFN induces 3α-HSDs in the liver, and these enzymes subsequently decompose DHT. These enzymes are also induced by alcohol via the Nrf2 pathway [20]; therefore, participants who habitually drink alcohol might have limited ability to induce these enzymes. In fact, plasma levels of DHT tended to decrease with broccoli sprouts intake, with the exception of participants who appeared to show alcohol-associated impacts on liver function (γ-GTP < 50 IU/L and ALP < 260 IU/L) (S1 Table)."
While Ozeph tries the liposomal form, which I’d still consider a worthwhile trial, I’ll buy a few boxes of broccoli sprouts and begin by eating the same amount (50 g) that the participants in this study did. At some point I intend to eat an entire container a day. What’s great about this is that I can buy these at the supermarket down the street, and I can begin tomorrow.