With aza I suppose you are referring to 5-aza-2’-deoxycytidine, which is Decitabine. What did you mean with “deca”? Btw, there are many substances that have been shown to be demethylating agents, not just two. So which ones do you try? I tried this one (IV procaine).
Most things in our body are highly conserved over millions of years of evolution, and here for a purpose. The whole methyl group system, comprised of methylation and demethylation processes, is absolutely essential for life. For example, methylation plays a key role during cell mitosis (cell division). If you start interfering with those processes too strongly or in the wrong way, you’ll likely quickly end up dead.
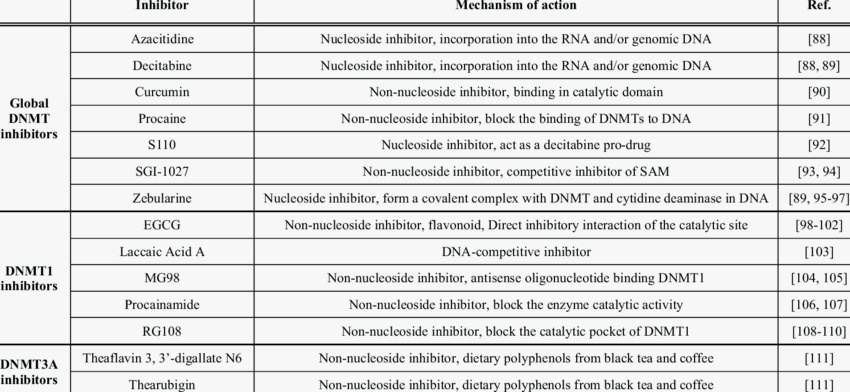
The big problem with demethylating agents such Decitabine, is that they are very powerful and unspecific, meaning they will act all over, also where we don’t want them to (which is in most places). Once we find out what to do, we will hopefully only want to target a few specific sites. CRISPR type approaches are more promising here. On the other hand we also have HDACi’s, which is what the article posted in this topic is about. There are many of those too, and some will only target specific HDAC classes, which is a little more specific, but still not great either.
Epigenetic changes can happen very quickly. I would guess that we are all genetically predisposed to a certain degree. Because of the highly variable nature of our syndrome, in genetics the phenotype of “PFS” (etc.) would likely be classified as what is called a “continous trait” (also known as a quantitative trait). A continuous trait is controlled by multiple genes. This would mean that multiple genes, in various dominant/recessive combinations, are predicting our syndrome. I very much hope that we will eventually get at least some hints in that direction from our GWAS research project. The continous nature would explain why some guys get it very mildly after a long time, while others get an extreme form after only one or few pills.
Very high level, I believe that the basic mechanism is as follows:
- Anti-androgenic action at the cell level causes an upregulation of the AR and induces epigenetic processes which keep AR-overexpression persistent
- Overexpression of AR and ARG’s (Androgen Responsive Genes) causes negative regulatory response, thereby silencing signals
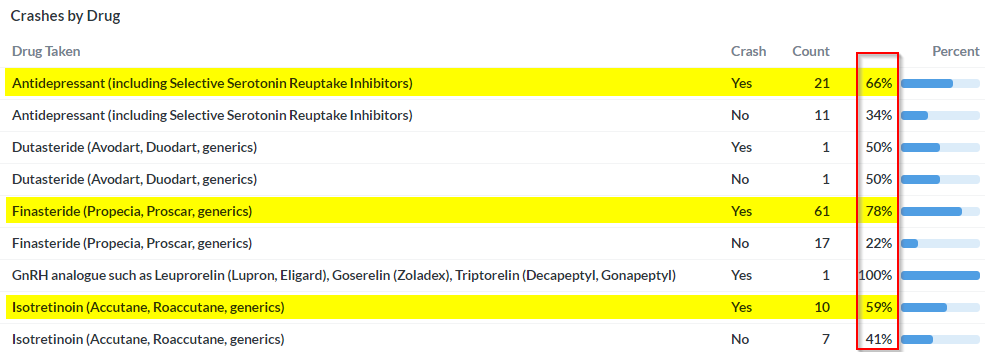
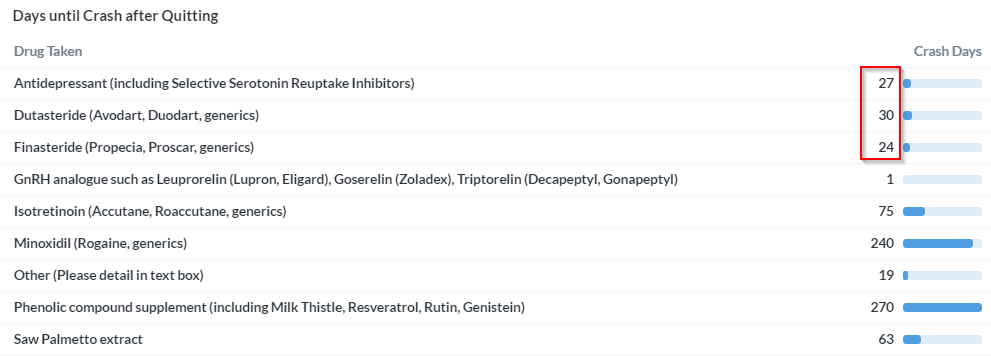
- Withdrawl of substance causes increase of AR activation, thereby exacerbating processes described in previous step. This is what we would call the “crash”
- AR remains in persistent state of overexpression, whereby further increases of androgenic action worsen the symptoms, while antiandrogenic influence will at least transiently improve the condition.
This hypothesis is supported by findings in the Di Loreto paper below and the basic underlying mechanisms of the above hypothesis have recently become quite well established in various publications. @axolotl, who unfortunately is very ill at this time, has been working on a comprehensive literature review in this regard.