
Why has no one tried aza or deca, the two demethylating agents? I think there is a high chance a lot of gene silencing is causing our problems. I know its risky, but people are commiting suicide over this condition. Things like valproate don’t effect even a percentage of things like these two agents. Honoustly interested.
Zadig, rest his soul, and I believe another PSSD forum member, supposedly acquired azacitidine but there seemed to be no report on the effect it had for either of them.
Does anyone know if it was actually trialed among any PSSD patients?
I am deeply into this stuff, even trying to make an appointment with a doc in india to do it on me. Zadig didn’t do it, he wanted to, but never did it. There was a report on pfs from a guy claiming he knew another guy that tried it for 4 days, got ill, and quit. The guy could get drunk after these 4 days again. He said this guy tried aza, which doesnt cross the blood brain barrier, deca does. And also he did it only 4 days, and the real demethylation takes place the 2nd cycle, so the 2nd 4 days (u cycle 4 days with a week in between). On the pssd forum no one has tried, I have pssd and read the forums there. I just find it unusual no one has tried it yet while people are commiting suicide. On the other hand its extremey hard to get, so I understand. I think it’s very promising, especially knowing methyl donors worsen us. I also found an artical talking about epigenetic changes taking place after drugs use/during withdrawal, this happened to me too. "Co-author Fal Yadid, of Bar Ilan University, added:
'Surprisingly, we discovered that the biggest changes in DNA methylation occurred not during the exposure to the drug but during withdrawal.
'During this period of withdrawal, hundreds of genes changed their state of DNA methylation including genes that were known before to be involved in addiction."
3 Likes
Thanks for the report. I was under the false impression that at least a couple PSSD patients had tried it. My fear is that to achieve a strong enough effect to reverse this condition, it may require an intolerable toxic dose.
There were also a couple reports of PSSD patients using valproate for its epigenetic effects. I believe one claimed recovery and another said it made some symptoms worse?
1 Like
well i found out that lower dose decitabine, so not high, is the best for demethylating genes. Going higher is even worse for demethylating as weird as it may sound. The only worries i have is that not all genes are effected good enough by the deca. On the other hand a guy on the pssd forum told me deca has been showed to be able to unsilence the dopa pathway, and Androgen genes. There is a guy who tried a combo of demethylating ‘‘agents’’ like valproate and some other stuff on the pssd forum, to mimic the effects of decitabine. Supossedly there is a pubmed article where they say they give this combo to cancer patients who don’t tollerate the real deal (deca) well. Another pubmed article claimed this combo doesnt even come close to the demethylating effects of deca. He said it recovered him for 60 percent, so that’s something.
2 Likes
With aza I suppose you are referring to 5-aza-2’-deoxycytidine, which is Decitabine. What did you mean with “deca”? Btw, there are many substances that have been shown to be demethylating agents, not just two. So which ones do you try? I tried this one (IV procaine).
Most things in our body are highly conserved over millions of years of evolution, and here for a purpose. The whole methyl group system, comprised of methylation and demethylation processes, is absolutely essential for life. For example, methylation plays a key role during cell mitosis (cell division). If you start interfering with those processes too strongly or in the wrong way, you’ll likely quickly end up dead.
The big problem with demethylating agents such Decitabine, is that they are very powerful and unspecific, meaning they will act all over, also where we don’t want them to (which is in most places). Once we find out what to do, we will hopefully only want to target a few specific sites. CRISPR type approaches are more promising here. On the other hand we also have HDACi’s, which is what the article posted in this topic is about. There are many of those too, and some will only target specific HDAC classes, which is a little more specific, but still not great either.
Epigenetic changes can happen very quickly. I would guess that we are all genetically predisposed to a certain degree. Because of the highly variable nature of our syndrome, in genetics the phenotype of “PFS” (etc.) would likely be classified as what is called a “continous trait” (also known as a quantitative trait). A continuous trait is controlled by multiple genes. This would mean that multiple genes, in various dominant/recessive combinations, are predicting our syndrome. I very much hope that we will eventually get at least some hints in that direction from our GWAS research project. The continous nature would explain why some guys get it very mildly after a long time, while others get an extreme form after only one or few pills.
Very high level, I believe that the basic mechanism is as follows:
- Anti-androgenic action at the cell level causes an upregulation of the AR and induces epigenetic processes which keep AR-overexpression persistent
- Overexpression of AR and ARG’s (Androgen Responsive Genes) causes negative regulatory response, thereby silencing signals
- Withdrawl of substance causes increase of AR activation, thereby exacerbating processes described in previous step. This is what we would call the “crash”
- AR remains in persistent state of overexpression, whereby further increases of androgenic action worsen the symptoms, while antiandrogenic influence will at least transiently improve the condition.
This hypothesis is supported by findings in the Di Loreto paper below and the basic underlying mechanisms of the above hypothesis have recently become quite well established in various publications. @axolotl, who unfortunately is very ill at this time, has been working on a comprehensive literature review in this regard.
11 Likes
Is the problem in the pssd guys also in the AR receptor?
If SSRIs mess with serotonine, which can also cause sexual dysfunction, could it be possible that serotonine receptors or serotonine levels in the brain played a role in their case?
Sorry, I am not a science guy, so I may be asking a stupid question without even knowing it. But this is a doubt that I have been having for some days.
1 Like
From literature, which @axolotl is compiling, this would appear to be extremely likely. Various antidepressant agents have been shown to exert strong anti-androgenic effects.
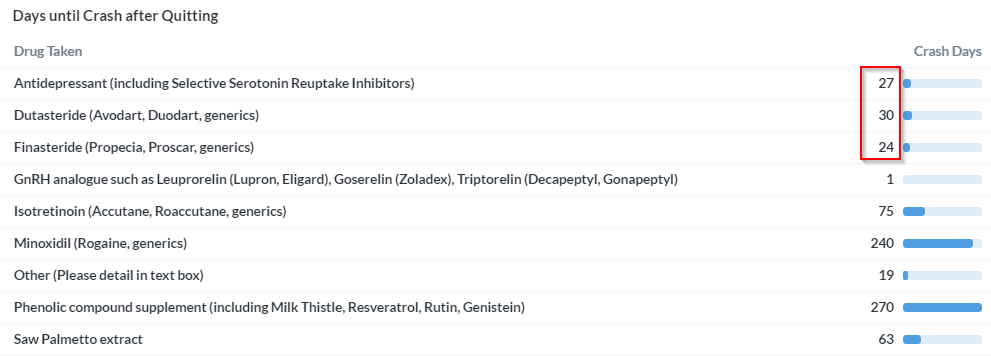
Look at the survey results concerning the crash. All three main drugs covered on this site are causing crashes, and even the number of days after quitting until the crash happens, are almost identical.
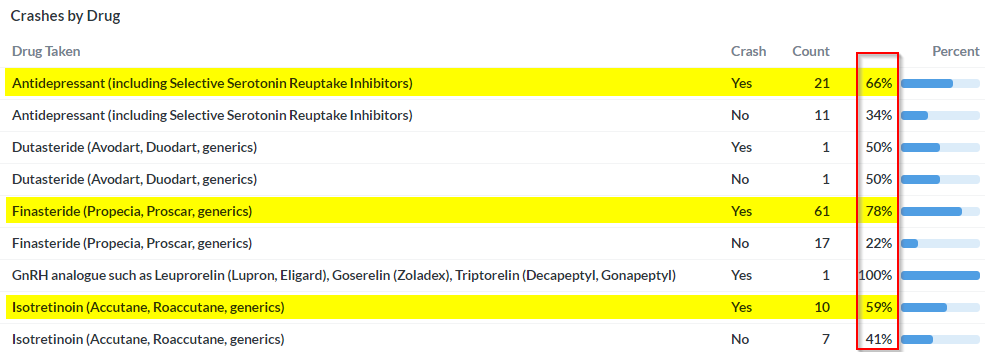
Furthermore, the symptom profile they are causing is nearly identical as well, check out our survey results in this regard.
As said, all three substances classes have documented to have strong, anti-androgenic effects. If this were not the same problem (i.e. same root cause), why would it’s presentation be practically identical? Howelse can the crash be explained, if not through AR overexpression? How can things like muscle wasting, penile shrinkage, skin changes, joint problems, increases in abdominal fat, gynecomastia, bone pain, perineum atrophy and other clearly documented anti-androgenic effects be explained by something like neurosteroids for example? At least to me, this makes zero sense. Of course, neurosteroids are involved, but I believe as a downstream effect of AR deregulation, and not as a root cause. Here also, Axo is working on producing the evidence from recent publications, which can plausibly explain how AR deregulation can lead to deregulated neurosteroids.
To all those who somehow seem to think that this rather obvious hypothesis is somehow uncool, just to be clear: From a strategic point of view, a common denominator is the best thing that can happen to ALL of us (PFS, PSSD, PAS, Lupron, etc.). If it is the anti-androgenic effect of these (and other) substances that is causing this, and we can make a plausible case (which Axo and I are working on very hard), this common denominator can be our ticket to substantial 7+ digit NIH level funding. Without funding in those dimensions, at least the research path is going to be a very rough one. Alternatively, if this hypothesis turns out to be completely wrong, and each drug is causing the same problem but via a different mechanism, I am afraid that no one will really care, as is the case now.
21 Likes
You know what? In the past I’ve said there wasn’t enough focus on actually finding a way to fix this on this forum. But my god. Propeciahelp progress is HARDCORE progress.
Thanks so so much for everything you do. 
9 Likes
If you’re reading this and haven’t done it yet, fill out the survey!
2 Likes
You are welcome. Axo, I and others have invested many thousands of hours of work into what we do, and also considerable financial resources. Everyone can thank us by simply supporting our projects. This means:
- Please take the survey
- and please contribute your 23andMe data
Even though both will not produce an instant cure, they will support our strategic work which will hopefully benefit you in the future. Btw, it would also be great to get more 23andMe data from PSSD and PAS patients. If we could manage to find some SNP’s which stick out in all three groups, boy this would be one hell of a smoking gun.
9 Likes
Yes there are other demethylating agents, but they are far from strong. Also refering to ur question about aza and deca. There exists azacitidine and decitabine (aza and deca). These two are different from each other. Decitabine crosses the blood brain barrier for example, azacitidine does not.
I do get that this is all risky ofcourse, but people commit suicide, and I think this ‘‘lottery’’ has to be given a chance if your other option is suicide. Some of us can’t come out of bed anymore/have very bad anhedonia, and I think for those people it might be a risk they are willing to take. If ur only problem is bad libido/bad erections, no, i wouldn’t try such a thing. I also do know about HDAC inhibitors, i used sodium butyrate for a while with some mild good effects, but got tolerance overtime.
Got here a list btw people might find interesting. As u can see the substance you tried is also on this list. It’s a non-nucleoside inhibitor sadly, and if I remember right, that is a must for sufficient results.
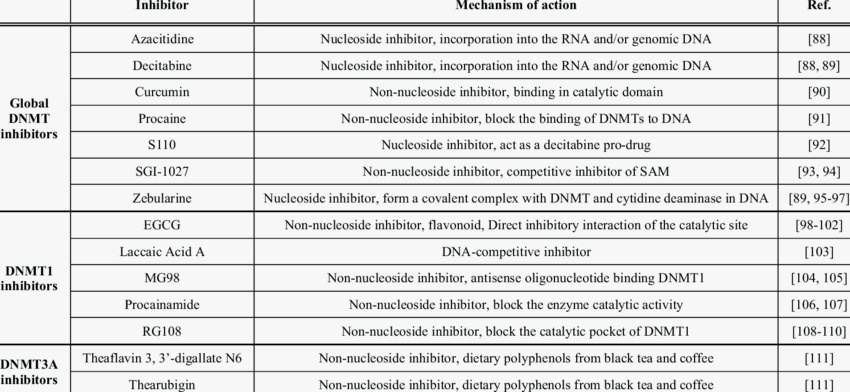
1 Like
I truly believe that the research has to be focused exactly on what you are focusing it, especially if we bear in mind the Di Loreto study findings.
But in my “battle” with doctors many of them have argued that these symptoms can also be caused by neurological problems (and I am not talking about those who told me to visit a psychiatrist, I am talking about doctors who saw the illness as something real that can obviously not be cured with antidepressants).
I don’t know to what extent this is true, because as I said I am not a scientist, but I can think of some neurological illnesses that have some of these problems.
It is also true that during the last months I have been strongly influenced by the last events in my life and some “medical professionals” too much.
I think we all agree that we need to push the AR overxpression theory until the end to see if this is really the cause, and in case it is, then analyze what can we do to solve it.
Then, if nothing is found, we can always start a different route. But it is clear that probably no one has done more research on PFS than you, so your opinion is certainly the most important in this subject.
2 Likes
If we are going to wait for the study to be finished, I bet you guys that it will going to take at least another 6 or more year and I am optimistic.
I would say, why not based on awor theory do not start some approach to down-regulate the AR with help of a professional in the mater instead of count the legs of a fly?
Otherwise we are going to die before any finding arrive.
Why do not try HDACI-bicalutamide for example under supervision of a forefront doctors in this matter ?
2 Likes
I don’t disagree that waiting for more research is pointless. But, which doctor is going to risk his/her license to give chemotherapy for a condition that is not even fully recognized by the medical community?
If I understand well the theory, trying to downregulate the Androgen Receptor with the current knowledge would be like trying to shoot an apple off a man’s head while being drunk and blindfolded.
As we get more information from studies, we may be able to remove the blindfold and aim at the apple with precision.
Are you willing to try it?
I am ready right now for HDACI-bicalutamide
1 Like
I know that I maybe will be criticized for bring back to the table the same issue , but here again
glucocorticoids can activate AR signaling in cells.
If you look in this subject there is a lot interaction between AR an glucorticoids, the more that I read abut the subject I do not have doub that Anonymous was recovered due the methylprednisolone some how it reversed on him the epigenetic change due FIN.
I am also willing to try methylprednisolone hight dosage trough vein, the only problem is to find the doctor willing to do it.
1 Like
Also there are herbs that can down regulate AR, some of those herbs had been used for cancer treatment as HDACI-bicalutamide.
For example baicalin and oridonin
baicalin or its aglycon baicalein, down-regulated the AR protein in the LNCaP cell line in a dose-dependent manner.
It make confuse because, it seem that down regulation of AR is like the same action of propecia did or no ?
Over here this study said:
HDAC inhibitors have been intensively investigated as AR suppressors.
our data supported the result that androgen including dihydrotestosterone suppressed AR transcript (data not shown)
Also this previous study have a long table with gene classification, gene function, cell, effect and supposed mechanism.
URGENT NOTE : BAICALIN AND ORIDONIN ARE IS NOT SAFE IT’S inhibit 5-alpha [reductase](https://www.sciencedirect.com/topics/medicine-and-dentistry/oxidoreductase)
Interentingly bicalutamide down-regulate AR but do not inhibit 5-alpha [reductase]
Bicalutamide does not inhibit 5α-reductase nor is known to inhibit other enzymes involved in androgen steroidogenesis
1 Like
I am trying to contact doctors in India as we speak to see if i can go there and get this treatment. It has to be done, we can’t wait for another X years without even knowing what explanation will be given to us.
3 Likes