From literature, which @axolotl is compiling, this would appear to be extremely likely. Various antidepressant agents have been shown to exert strong anti-androgenic effects.
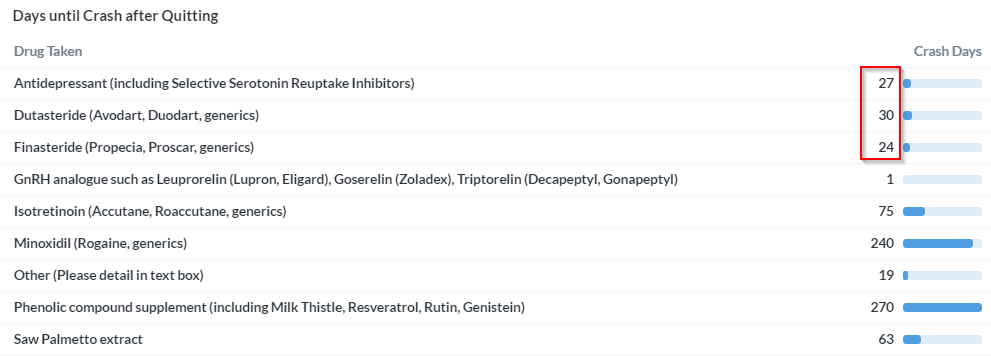
Look at the survey results concerning the crash. All three main drugs covered on this site are causing crashes, and even the number of days after quitting until the crash happens, are almost identical.
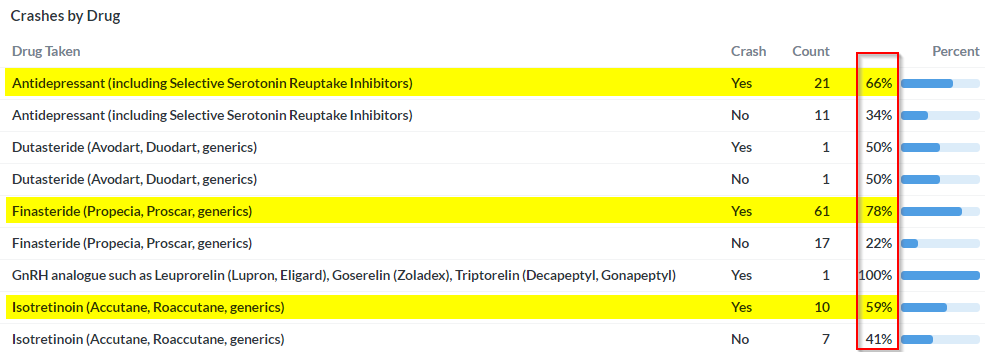
Furthermore, the symptom profile they are causing is nearly identical as well, check out our survey results in this regard.
As said, all three substances classes have documented to have strong, anti-androgenic effects. If this were not the same problem (i.e. same root cause), why would it’s presentation be practically identical? Howelse can the crash be explained, if not through AR overexpression? How can things like muscle wasting, penile shrinkage, skin changes, joint problems, increases in abdominal fat, gynecomastia, bone pain, perineum atrophy and other clearly documented anti-androgenic effects be explained by something like neurosteroids for example? At least to me, this makes zero sense. Of course, neurosteroids are involved, but I believe as a downstream effect of AR deregulation, and not as a root cause. Here also, Axo is working on producing the evidence from recent publications, which can plausibly explain how AR deregulation can lead to deregulated neurosteroids.
To all those who somehow seem to think that this rather obvious hypothesis is somehow uncool, just to be clear: From a strategic point of view, a common denominator is the best thing that can happen to ALL of us (PFS, PSSD, PAS, Lupron, etc.). If it is the anti-androgenic effect of these (and other) substances that is causing this, and we can make a plausible case (which Axo and I are working on very hard), this common denominator can be our ticket to substantial 7+ digit NIH level funding. Without funding in those dimensions, at least the research path is going to be a very rough one. Alternatively, if this hypothesis turns out to be completely wrong, and each drug is causing the same problem but via a different mechanism, I am afraid that no one will really care, as is the case now.