
Keep us posted about sulforaphane!
1 Like
Ok. So body odors do have something to do with pfs symptoms. My body odors are gone again. So yes, it may have to do with taking both Pine Pollen and Horny Goat Weed at the same time. That’s a finding by itself (for those interested in having to put deodorant. Lol)
I think Sulforaphane is not going to give spontaneous response like taking 5-HTP or L-Dopa. (or a testocaps, they always gave me a rush). I’m at 200 mg a day now. If after sometime I still don’t see effects, I’ll try with DMSO. Truth is, I do have some feelings that seem to come from the past. But it’s not obvious at this point.
I’ll keep you posted.
Confirmed for body odors. If I take both Pine Pollen and Horny Goat Weed things return to normal.
About Sulforaphane:
I had a bad night of sleep last night. 4/10 . The weird thing is I was tired at bed time and went to sleep fast but I just kept waking up and falling in a light sleep, dreaming all the time. The dreaming zombie state as I call it. I usually feel not rested after a night like that.
I made five changes in my regimen:
I’m taking Creatine. It could be it but it’s said to be to be non-stimulant and can be taken even before sleep. (for non-pfs people anyway). It boosts testosterone and androgen, but only if you exercise which I haven’t done that much. I’m in the load up period and still suppose to load up for 3 days but I’ll just take the maintenance dose for now until I can fix my sleep.
I’m taking 4.5 mcg of Boron if adding my multivitamin. I doubt this makes a difference. The upper limit is 20 mcg. 10 mcg is used to boost testosterone.
I’m taking Horny Goat Weed once in the morning. Could be that, but it’s supposed to affect testosterone and sex drive, not sleep. Plus I stopped One day and sleep was bad anyway.
Sulforaphane. Yesterday I took around 300 mg. It did make me feel calm yet confident and motivated during the day, and I was sleepy before bed. But I slept bad while just a week ago, before any changes in my regimen, I was saying sleep was getting better. ( 8.5 or 9/10) Today I will reduce to less than 100mg and see what happens.
Sleep patterns: The 2 months school vacation just started in Thailand last week. My sleep patterns are all messed up. I go to sleep at the same time but wake up at 8 instead of 6:30. So instead of 8 hours, I get 9 and half and that, by itself, has always caused bad nights on the next night.
So I’ll fix my night pattern, that’s the best educated guess I can take as oversleeping has always resulted in bad sleep the next night. I’ll cut down Sulforaphane to less than 100mg until I get better sleep. If after fixing my sleep patterns I still can’t sleep good, I’ll have to cut Sulforaphane.
Following my regular rules,Sulforaphane didn’t significantly make me feel better while I did have bad side effects. I still cannot attribute those to Sulforaphane but after fixing my sleep pattern, I’ll know what’s the cause of this bad sleep.
Hi. Do you have any study regarding this fact? Thank you
I looked again and I have been wrong. My sources were from a hair loss forum and it was incomplete.
5-ar produces DHT and 3a-HSD eliminates DHT in the muscles. Both are working together and are essential to produce ALLO and other important neurosteroids.
However, as far as I’m concerned in raising 3a-HSD levels (with Sulforaphane), I will also want to raise 5-ar levels to make sure I have normal DHT.
And to answer to myself on this post, I did fix the sleep patterns and slept better. Sleep is no longer an issue as long as I don’t sleep more than 8 hours.
I decreased Sulforaphane to 50 mg a day which seems to be adequate and I found that it was either improving the effect of Tyrosine, or using it at a much faster pace. As a result, after taking Sulforaphane I stopped having brain fog and became more focused. I also have an inner calm I haven’t felt for a very long time (years) but I ended up depleting my Dopamine and Serotonin. (felt demotivated, unhappy, depressed, and unsure of myself)
So I continued to take 5-HTP 100 mg, L-Dopa 350 mg, L-Tyrosine 375 mg, all three two times a day and I also take half a dose of St-John’s worth (300 mg, it’s a plant extract) which is a unique non selective, all neurotransmitter re-uptake inhibitor to prevent my Tyrosine, Serotonin and Dopamine from being depleted.
5-HTP and St-John’s Worth are dangerous together so I monitoring how I feel carefully, taking only small doses of that herb and I’m ready to stop it the moment I feel a dopamine or a serotonin rush (after months of testing those, I know how too little or too much of those feels like). Stopping St-John’s Worth would let my body flush the extra neurotransmitters. At the same time, to make sure, I would also stop the intake of the neurotransmitter that seems over-abundant.
And considering Tyrosine seems to have a greater effect, I’m taking a small dose of Phenylalanine (350mg per day) to prevent depleting that one as well. Tyrosine and Phenylalanine are the precursors of the neurosteroids responsible for regulating the nucleus acumbens, where all the Dopamine receptors are located. (I could name those neurosteroids, they have long, funny chemical names that look like they come from a Star Trek episode)
For a second day in a row, I felt more normal than I did in years. Even more normal than when I was taking fin (in the end, it was making me very irritable).
I’m not suggesting any of you try what I’m doing. As a matter of fact, it can be dangerous. I’m just documenting what I’m doing and the effects it has on me.
I’m looking forward to a good night of sleep and a fully motivated, productive day tomorrow.
I’ll keep you posted (more on Amino Acid For neurological symptoms)
3 Likes
where are you guys reading that pfs has low 3a-HSD activity?? data we have points to the other direction
https://sci-hub.tw/https://doi.org/10.1016/j.jsbmb.2017.04.003
also like @Ozeph said 5ar and 3a-HSD are antagonists why would you want to increase the latter?? makes zero sense to me
1 Like
My statement that 5ar and 3a-HSD are antagonist is incorrect. I got it from a dubious source and could not verify it from trustworthy study.
Here’s where it says Allopregnanolone is particularly affected by pfs: Couldn’t find it online so here’s a copy:
The metabolism path is incomplete, it’s both 5ar and 3a-HSD that transforms progesterone and Deoxycorticosterone into it metabolites. Considering many of us shows GABA abnormalities but still have 5a-DHT I theorized that 3a-HSD was the one missing.
Allopregnanolone – How to Increase the 5-Alpha-Reduced Allopreg
In Neurosteroids by Tyler SJanuary 30, 20174 Comments
Allopregnanolone (allopreg for short) is a powerful neurosteroid that has been in the headlines recently ever since the deadly “post finasteride syndrome”. Allopreg is considered a neurosteroid that has numerous neuroprotective properties that range anywhere from the importance of the regulation of emotion and its therapeutical use in depression and anxiety may not only involve GABAergic mechanisms, but also includes enhancement of neurogenesis, myelination, neuroprotection, and regulatory effects on HPA axis function. When your body is under stress, allopregnanolone acts as the body’s natural tranquilizer or anti stress mechanism to help dampen the response [here]. It is highly involved in many mental disorders including mood disorders, depression, anxiety, sleep disorders and seizures. One of allopreg’s main role in the central nervous system is activating the GABA (A) receptor (taurine also does this) which provides many of those anti stress properties [here].
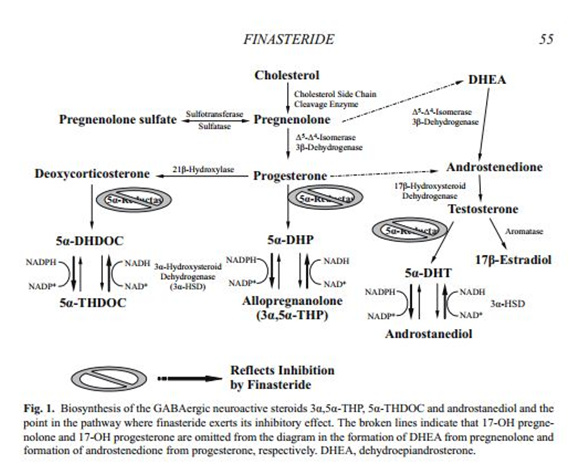
Now if you take a look at the chart above, you can see how finasteride (or any 5 alpha reductase inhibitor) can negatively impact the proper synthesis of not only allopregnanolone but also another important neurosteroid, tetrahydrodeoxycorticosterone (another anti stress mechanism). Allopreg is synthesized from progesterone which then gets converted into the direct precursor, 5a-DHP (5a-dihydroprogesterone).
Through the series of coenzymes (NAD/NADH) allopreg is now established in the brain.
Now to put into perspective how powerful allopreg really is- it’s actually under development under the name “Ganaxolone” for the treatment of seizures, anxiety, epilepsy, Alzheimer’s, Parkinson’s etc. The difference is that Ganaxolone is allopreg’s synthetic brother [here].
Why are the mental effects (anxiety, memory loss, poor stress tolerance) of finasteride or any 5 alpha reductase inhibitor so severe? Well, there is a significant amount of 5AR expression in the brain and it fits in line with anything that disrupts that function like finasteride which absolutely destroys allopreg in the brain along with MANY other neurosteroid/steroids in the body besides just shutting down the conversion of DHT only. It was hard to find this study especially on male humans, but the results are pretty astounding [here].
This is only after 5 months, also keep in mind that the study notes 5mg of finasteride, but 1mg vs 5mg are pretty much the same in terms of 5AR inhibition in the body and brain [here].
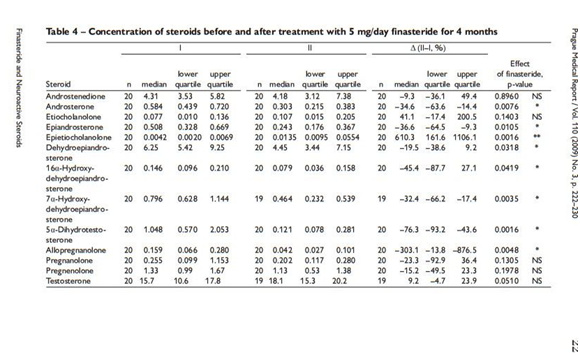
As you can see, anything with a negative (-) number is taking a hit- allopreg being the absolute worse. So much for just being DHT only.
Alright, enough bashing 5ARi’s now it’s time to take a look at how to optimize allopregnanolone both for optimizing mental properties long term and also for anyone recovering from 5 alpha reductase inhibitors.
So as noted from the first master chart above that displays the entire hormone cascade, there a few different ways to increase neurosteroids in general but mainly allopreg:
• Oral pregnenolone at higher doses was shown to increase allopregnanolone significantly.
• Caffeine was shown to increase pregnenolone, progesterone and allopreg in the brain [here]. The trick with caffeine is to take it after eating food and enough sugar to avoid the stress (cortisol) response when lack of glucose is available.
• Progesterone, which is one of allopreg’s precursors can raise allopreg levels [here]. If you are a male, probably wouldn’t go to high on the dose to avoid any potential anti androgenic effects or just simply supplement with oral pregnenolone instead to let your body regulate the conversion of progesterone synthesis.
• Supplementing with the direct precursor to allopreg, 5a-DHP works pretty damn well too. It’s hard to find, but one legit vendor does offer it [here]. I have experimented with 5a-DHP on my pet rat and the effects seem almost identical to a benzodiazepine- without the foggy memory issues which means that it is getting directly converted into allopreg.
• Glycine is another amino acid that can increase allopreg [here]. I found doses 6+ grams was best used before bed.
Another quick tip is whichever method you decide to take, supplementing with a small amount of niacinamide concurrently with any method will help enhance the conversion of neurosteroid activity by increasing the coenzyme (NAD/NADH) [here].
Allopreg in the bio-identical form is not available from any legit vendors after doing some quick searching around- mostly vendors looking to sell to a business (commercial use). Leveraging the precursors would actually be safer in optimizing serum allopreg levels since your body can regulate it better.
Ozeph’s Note: I tried Pregnenolone at high dose. I became hyper and unbalanced and it addictive. It has to be tapper down slowly. I also tried (and still using) Sulforaphane as for me it’s very efficient at clearing brain fog and keeping me motivated. I’m also singing songs in my head while taking it, which I don’t do when not on it. I can say my ability to feel happy is greater with Sulforaphane. Studies shows increased 3a-HSD when taking Sulforaphane.
5 Likes
please post the link to this study so people can understand the methodology and interpret it themselves
the one i posted measured specifically cerebrospinal fluid e.g brain levels and we have evidence of excess allopreg/gaba-agonism in PSSD too
2 Likes
Got positive changes with glycine, but these improvements diminish very quickly. I got noticeable Increase in ‘‘visual’’ libido and stronger boner. And 6G of glycine making my body feel tense.
1 Like
The thing is, the study you posted would reflect what happens while taking an SSRI.
Is there any evidence that this is the same as PSSD?
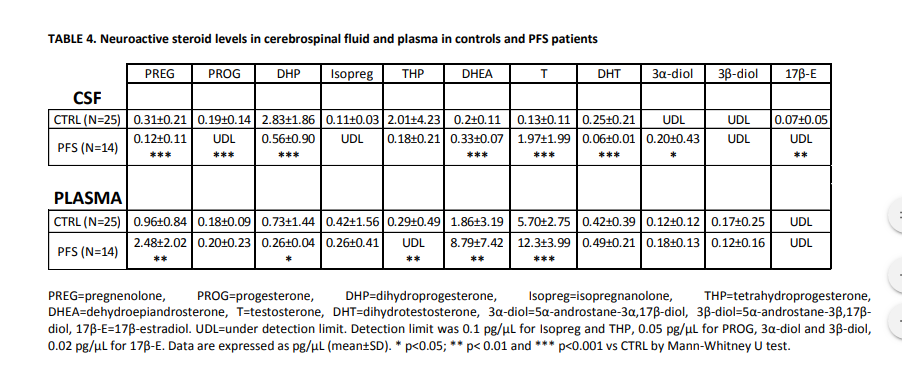
Many PFS patients have normal serum DHT levels, for instance. This was also the case found in Melcagni’s study.
I don’t the the typical effect of a medication during use can be translated to apply to these post-drug conditions.
1 Like
I don’t have the link to the study. Maybe it can be found by google searching the first paragraph.
The study is about pfs, with normal DHT levels. It points out at a lack of 5ar as the reason for not having Allo, I just wanted to add that it’s both 5ar and 3a-HSD that creates Allopregnanolone and 5a-THDOC.
I agree with Dubya_B that the suggested treatment for increasing Allo is for normal people (or non-pfs pet rats) and may not work for pfs patients. It didn’t for me.
which study?
i feel its important to note patterns like high dhea / low androstenedione in PFS, its the exact opposite in hyperandrogenism
why are we even talking about serum levels?
of course not, we are the perfect example
1 Like
That’s what I thought at first as well until I learned that 3b-diol inhibits growth of prostate cancer cells and that low 3B-HSD can mean low 3b-diol
Low 3b-diol is actually the suspected cause for why taking DHT inhibitors can make you have a greater chance of having high grade prostate cancer after taking DHT inhibitors
So what was the end result with taking Sulforaphane to increase 3A-HSD?
Did it work ?
Also did you ever test your 3b-diol, 3a-diol or Androstenedione levels to test for evidence of low 3A-HSD prior to this experiment?
If no what is leading you to believe you have low 3A-HSD?
This is something I’m interested in because I have flagged low 3b-diol, almost flagged androstenedione and lowish 3a-diol.
I suspect I’m low in 3A-HSD
I’m in Thailand and I did no blood test. I acted on a theory.
From what I can tell, Sulforaphane boosts mind clarity and focus but depletes L-Tyrosine, Dopamine and Serotonin.
I have no evidence that it did anything to my 3a-HSD, or if it did, that 3a-HSD improved my insomnia or stress levels. 3a-HSD + 5-AR + Progesterone = Allopregnanolone which should regulate GABA a receptors, fix insomnia and a whole bunch of other things.
However, that is if every part is doing its work correctly which I now doubt. Some parts seems to have gotten long term damage. What works best for me is very low carbs diet, with lots of saturated fat and some mono unsaturated, and lots of fat cuts of meat. Then some exercise and weight lifting on top on this. I believe this is repairing the long term damage as I have seen improvements on every symptoms. Most of them are gone actually. (after 13 months of diet)
No easy button for this one. I don’t think a pill will do the trick. I had to take the hard path.
So you contribute the improvements you got to increase in allopreg ?
Did you know you can take 5a-DHP which converts directly to alleopreg?
I may try to get 3b-diol from a research lab and take it straight some day.
I attribute it to having more Beta-HydroxyButyric acid in my blood by doing a ketogenic / carnivore diet.
It lowers Glutamate (excitatory), rises GABA (calming) and some research indicates it may repair damage done to the DNA although I can’t say if it’s true or not.
I don’t know if it influences Allo. I looked at 5a-DHP and it seems to work but it’s dose dependent.
If you do try it, please let us know the results !
Any update on the Brussel sprout regimen, captain?
My latest research and what I am looking into involves the enzymes 3a-hydroxysteriod and 3B-hydroxysteriod. I forgot that we already started going down this path until I found this thread again. @Dubya_B I agree with what you and I also believe that Fin and Dut can effect the 3a-HSD and 3b-HSD enzymes by binding NADPH. I also believe that the way Fin and Dut effect 5AR is by binding NADPH. We have been led to believe for many years that 5AR inhibitors “inhibit or decrease the actual 5AR enzyme” I don’t believe that this is correct. Instead I think Fin and Dut temporarily inhibit T-DHT conversion by preventing the 5AR enzyme from being able to use it’s cofactor NADPH to catalyze the conversion of T-DHT. I believe that the main difference between people who develop PFS and people who don’t comes down to issues with binding NADPH and that any enzyme that needs NADPH to catalyze it’s function has the potential to be effected.
“Mechanism-based inactivation of 5α-reductase type 2 by finasteride showing a hydride reaction occurring between finasteride and NADPH that results in a covalent bond between finasteride and the cofactor. [R = -C(=O)-NH2; PADPR = 2’-phosphoadenosine-5’’-diphosphoribose; A-H = TYR58.7] Finasteride in relation to NADPH while bound to 5-beta-reductase, note the distance between the hydride on NADPH (purple) and the sp2 hybridized carbon on finasteride (green)”
https://cbm.msoe.edu/crest/posters/2015CUWSP/15finasteride.html
“Finasteride is a selective 5α-reductase type 2 inhibitor that reduces plasma 5α-dihydrotestosterone levels and shrinks the size of the prostate (7). … Subsequent to inhibitor binding*, there is hydride transfer from the NADPH cofactor to the Δ1-2-ene double bond of finasteride”
“Testosterone is irreversibly converted in a nicotinamide adenine dinucleotide phosphate (NADPH)-dependent reduction reaction to the most physiologically active androgen 5α-dihydrotestosterone (DHT)”
“Circulating testosterone diffuses into prostatic cells, where it is irreversibly converted into the more potent androgen DHT via the NADPH-dependent reduction catalyzed by the steroid 5α-reductase type II and, to a lesser extent, by steroid 5α-reductase”
“finasteride (Proscar®; Propecia® [Merck, NJ, USA] Figure 1), which was approved for benign prostatic hyperplasia (BPH) and alopecia, respectively [203], and the dual steroid 5α-reductase (type I and II) inhibitor dutasteride (Avodart® [GlaxoSmithKline, UK]), approved for BPH [204], mediate their effects by mechanism-based inhibition of steroid 5α-reductase type II”
“The mechanism of 5α reductase inhibition is complex, but involves the binding of NADPH to the enzyme followed by the substrate”
So clearly Fin and Dut are effecting NADPH. They are not just “inhibiting the 5AR enzyme”. With this being said it makes since that every enzyme that need NADPH as a cofactor will be effected
I would also like to see some studies that support the idea that 3a-HSD and 5AR are “mutual antagonists”. This theory is interesting.