Sorry this has been a very very long read and I have very long mentally exhausting workdays.
You’re hypothesizing that high progesterone levels (in the brain) are the likely reason for PFS/PAS? I’m just trying to draw a conclusion out of all the walls of text above.
1 Like
Hi there,
No problem, if you just read the first few paragraphs I have written a summary of the theory. But yes I think it is plausible that PAS is linked to persistently elevated levels of progesterone either during treatment which causes some form of dysfunction which needs to be corrected or these changes in progesterone production continue after stopping treatment and so remains a problem resulting in PAS.
This theory relates to more to PAS as the research is linked to metabolites of isotretinoin and progesterone. However I have seen a theory which links PFS to progesterone as I believe finasteride does have some progestagen activity but I haven’t spent much time looking into that yet.
1 Like
one pillers break this theory immediately. All hormones were measured thousands of times by majority of users, there is no single hormone that would indicate the cause of the PAS.
I haven’t heard of many one pillers who have full blown PAS but this in no way breaks a theory. Just reverting to one pillers can break this theory, on that logic one pillers could break every plausible theory. Can you think of a single theory which would make sense in the light of supposed one pillers? Does that mean all theories are not legit? There is certainly a theory which is correct and works in spite of one pillers.
I imagine one pillers who develop full blown PAS are very much an exception to the rule (a rarity), I am sure these individuals do exist but they are likely to have some kind of extreme sensitivity to the effects of PAS. They may have multiple gene variants, each of which makes them more sensitive to developing PAS than the average person. Thus the combination of these gene variants together makes these individuals hypersensitive, so that they develop full blown PAS very quickly. In this light, these individuals do not disprove this theory.
What if a person has multiple gene variants such as:
- A variant which greatly reduces the ability to eliminate Isotretinoin metabolites from the body.
- A variant which greatly increases progesterone receptor expression or binding capacity.
- A variant which greatly increases progesterone production in response to isotretinoin metabolites.
If you imagine all three of these in a single individual, it becomes possible for just a few pills to lead to PAS. Again though, these individuals would be very much rare cases and from what I have read, they do appear very rare as I haven’t heard of any, I have only heard of PFS people who took a single pill.
Again how do you explain why PAS can develop after a single pill in some people but it can also develop only in a second course of isotretinoin, meaning individuals take an entire course of isotretinoin but do not develop PAS.
Yes thats where it works on progesterone, glucocorticoids and HPA, i feel like its reset something in me.
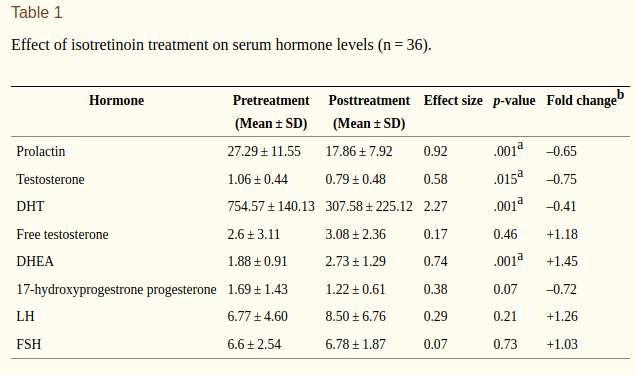
Just something to add to the conversation about DHEA:
A. Feily et al. , “The effect of low-dose isotretinoin therapy on serum androgen levels in women with acne vulgaris,” Int J Womens Dermatol , vol. 6, no. 2, pp. 102–104, Nov. 2019
1 Like
Interesting, it seems that HPA over-activity is likely to be a common effect of Isotretinoin.
1 Like
M. Cappel, D. Mauger, and D. Thiboutot, “Correlation Between Serum Levels of Insulin-like Growth Factor 1, Dehydroepiandrosterone Sulfate, and Dihydrotestosterone and Acne Lesion Counts in Adult Women,” Arch Dermatol , vol. 141, no. 3, pp. 333–338, Mar. 2005
M.-J. Chen et al. , “High serum dehydroepiandrosterone sulfate is associated with phenotypic acne and a reduced risk of abdominal obesity in women with polycystic ovary syndrome,” Human Reproduction , vol. 26, no. 1, pp. 227–234, Jan. 2011.
High levels of adrenal androgens appears to also be associated with acne. Interesting that their levels actually rose during treatment.
The question of whether similar changes are present in symptomatic post-Accutane patients remains.
1 Like
@Dubya_B and anyone else with contacts.
Can we get in touch with a doctor who can advise a dose for men? And inform us of the effects mifepristone will have on men.
Do you know anyone who can help us with these points ASAP?
Likewise I am interested in hearing about the potential for mifepristone. There are bound to be some risks involved, so this needs to be a carefully-explored thing.
I already have mifepristone ready since last night, thats why i wrote ASAP. If anyone knows any endocrinologist, lets get these points clarified.
I browsed a bit of pubmed and mifepristone is also used for type 2 diabetes in men at 600mg (in trials afaik). So it should be okay, but a bit of advice will go a long way.
Anybody?
2 Likes
Hello PAS,
Where did you get the mifepristone? I am still waiting to get some.
I don’t want to give medical advice, some on this forum have warned about being careful with mifepristone.
I personally think, taking mifepristone at a dose of around 750mg daily for a week shouldn’t pose any serious harm or threat. You will likely get some side effects such as water retention etc. towards the end of the week but these will subside when you finish.
Others have taken similar dosages and have been fine.
Hey man
Waiting means you’ve ordered it? I got it OTC as abortion pills. But it’s tough to get a good quantity, one pill is 200mg and they don’t stock much. I got a lot of shady looks yesterday
How did you arrive to 750mg as the dosage? Who are these others? It would be good to know their thoughts.
Do you know any endocrinologist? Even a phone call with them would help. Especially if they know your history.
1 Like
Hello, which post is this referring to?
Hi there,
I haven’t been able to get any yet nor have I had a good opportunity to take some as I plan to use when I have 1-2 weeks with no responsibilities. I will post when I if I do though. I think someone on the other thread mentioned they took some.
1 Like
I had a retrogade ejaculation at the 3rd day of taking Accutane that day still haunts me after 7.5 years. Retrogade thing healed back a day after but my PAS ( low semen) didn’t. I also probably had numb orgasms but i didn’t realize it, years later when it got worsened and worsened i joined this site, 2018 i think. I was 18 i think when i joined here.
No mental symptoms except self driven anxiety and OCD.
Weird, i also had very dry and white, falling out skin and back pain on the second day. These symptoms occur in people after months of treatment. These two also went away after a week. Im a hell of an interesting case for sure. Lmao. I wish i could find what is my issue. Seems like prostate. I want to do that Gene test @Gord shared.
Please check out that test and do it immediately if you PAS guys in are UK we need to see our gene predisposition! This is very important.
Might be useful as a note, I have had dheas tested it came back too low.
So might be just me or maybe things go south for some.