
Hello. I dont know much about accutane but i wanted to let you know my findings of pssd. In pssd, there is an increase in allopregnanolone causing the downstream effects. Ssris directly increase the conversion of 5a DHP to allopreg by over 40 fold. In unlucky cases the anti estrogenic effects of 5a DHP which will get up/downregulated will cause a hormonal rebound that damages mitochondria in sensitive tissue. On top of that allopregnanolone likely stays high causing high gaba and low glutamate. If its not allopregnanolone thats high there is likely genomic effects of 5a dhp on gaba receptor expression. The problem is there is only 1 class of RCs that can inhibit neurosteroid potentiation on the gaba receptors.
1 Like
You should try and fully write out a theory about this, so people can better understand what you think has happened.
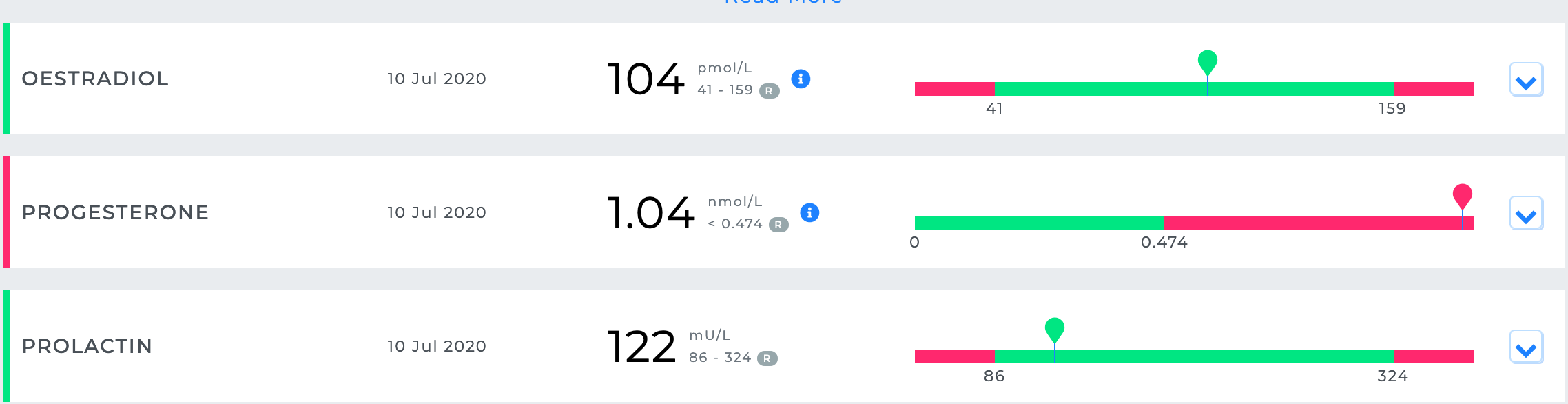
Hey guys, I just thought it would be worth giving an update here, firstly I had a blood test earlier this year. Of all the blood results to come back, my progesterone was at the top of the range for the test and was the only abnormal result. I have attached a screenshot below. This result is likely irrelevant anyway, as I imagine progesterone levels may be up-regulated in the brain only and not in the rest of the body. But it is still interesting.
However what is much more interesting is that a user on my own forum claims to have had a complete improvement of various symptoms including sexual issues (libido, erection strength), and said he felt pre-accutane after taking 700mg of Mifepristone for 7 days. This is very interesting considering what I have written in my theory above as I suggested mifepristone could be worth trying. I am currently trying to contact this user to get further confirmation etc. Here is a link to the page (Disclaimer: I am not trying to promote my own forum here, propeciahelp forum has much more user engagement and content, I was planning to close my own forum months ago, so I am happy I didn’t considering this users’ post)
2 Likes
Hi, what dose of mifepristone did you take and how many did you take it? Was it for one day or two days etc.? Did you you cycle it?
The more I think about this theory, the more it makes sense to me. Studies have shown that Isotretinoin significantly increases progesterone production in human glial cells (brain cells) in a significant manner. If these genetic changes persist after stopping Isotretinoin (which is very possible given the fact brain cells are non-dividing cells), then people with PAS may be stuck with high levels of progesterone production which is specific/localised in the brain tissue. This progesterone would then be effecting neural signalling in the brain.
Maybe the reason people get PAS relates to genetic differences in the progesterone signalling pathway such as progesterone production or the type of progesterone receptor, thus making them more or less sensitive to changes in progesterone. Or as has been stated before, people with PAS are less capable of metabolizing Isotretinoin and clearing it from the body, thus they develop PAS as the levels of Isotretinoin get much higher than other individuals and so the changes in progesterone signalling in the brain are much stronger and lead to long term changes in gene expression and progesterone signalling.
This helps to explain why sexual dysfunction affects females and males at the same rate in PAS as high progesterone has been shown to suppress sexual function in both males and females. In addition, the suppressive effects of progesterone on dopamine signalling, help to explain most if not all of the mental side effects such as depression, anhedonia, loss of motivation, de-personalisation, fatigue, apathy, blunted emotions, poor cognition, loss of memory etc. As high levels of progesterone signalling would be capable of suppressing dopamine signalling in areas of the brain such as the striatum and mesolimbic pathway, signalling in these brain regions plays a significant roles in all of the above brain processes.
Many people have noted that many of the symptoms of PAS are similar to the negative symptoms of schizophrenia. These symptoms are all thought to dopaminergic hypofunction (decreased signalling) in areas of the brain such as the mesolimbic pathways.
I have always been interested by the fact that PAS appears to also have significant effects on female sexual function, this has always made me skeptical of the idea that androgen signalling is the main culprit. Androgen signalling also appears to work fine in the rest of the body such as the muscles etc. Though testosterone is thought to play a role in female sexual function, estrogen is known to be the most important. Thus it seems strange to me, that changes in androgen signalling would have such strong/pronounced effects in females with PAS. I may need confirmation on this, but I imagine females with severely reduced androgen signalling would still have some degree of sexual function provided estrogen was normal. Note that many women with PAS report symptoms such as vaginal dryness, from looking online it seems that symptoms such as these are related to pre-menstrual syndrome and are due to low estrogen signalling and high progesterone signalling. Given this, high progesterone signalling in the brain can help to explain female sexual dysfunction in PAS, and may make more sense then issues with androgen signalling.
Another interesting thing to note is that there are clear links between progesterone and joint pain. I often notice that people report joint pain as a symptom, many women who report sexual dysfunction also report things like joint pain and vaginal dryness.
The progesterone theory offers a highly plausible cause of PAS in my opinion, that must be investigated. I am yet to see a theory which is plausible based on research in human cells such as glial cells and which links male and female sexual dysfunction as well as helps to explain how the other mental side effects could arise alongside sexual dysfunction.
One way to investigate this theory would be to try measure progesterone levels in brain, this may be possible by using some sort of progesterone tag in the brain and then measuring the levels of progesterone that way. Ultimately, if this theory is correct, treatment would focus on reducing progesterone signalling in the brain to bring signalling back into a normal equilibrium.
3 Likes
I just want to chime in and point out that I believe mifepristone also acts as an AR antagonist. What if the improvements that @Ronnie99 got came from that effect rather than from antagonizing progesterone receptors? It would be in line with improvements that other members here have had when taking anti androgens of various kinds (5ari, ar antagonists, etc.). I’m no expert anyway, just an observation.
1 Like
Hi, yes this is certainly possible however the primary activity of mifepristone is not an AR antagonist, it is a PR antagonist. Additionally, if this were true, then we should see extreme improvements in those who use potent androgen receptor antagonists. I don’t have time to look right now but could you link some studies which show mifepristone is a strong AR antagonist please.
The AR may be the main culprit here but I can’t help but feel like its possible that people have focused entirely on the AR as it makes the most sense but have overlooked progesterone and the PR.
I don’t think many people on this forum have used AR antagonists because it’s obviously very dangerous and can result in worsening of symptoms. Anyway, you could certainly be right, I don’t know enough to comment.
Here are a couple studies that demonstrate it’s effect as an AR antagonist:
https://bjui-journals.onlinelibrary.wiley.com/doi/full/10.1111/j.1464-410X.2008.07509.x
2 Likes
Thanks for posting, this is interesting and definitely worth considering. However, I still think the effect of mifepristone on progesterone signalling or the HPA axis is more likely to explain its beneficial effects. But I could of course be wrong.
2 Likes
Are you going to try Mifep yourself? Please keep us posted if you do.
1 Like
Very interesting thread, I think it is one of the most thought out theories we have.
1 Like
Hi Cooper, Yes provided I don’t find any strong reasons not to. I feel like I have to take a risk and give it a go especially when there are multiple lines of evidence which suggest it could help.
I will also trial it at a high dosage to ensure that if it can help us, I will know about it. I am currently in the process of obtaining some.
3 Likes
Just to add, here is another significant study which found isotretinion can cause HPA axis over-activity. Mifepristone was able to restore the HPA dysregulation. It is also significant as HPA dysregulation is linked to depressive symptoms, anhedonia, cognitive issues, diminished libido, hair loss etc. Thus this is another reason why Mifepristone could be worth trying even if my progesterone theory is incorrect.
Something that is also interesting about this theory is that high DHEA is a often a symptom of HPA over-activity. When I had blood tests my DHEA was abnormally high (off the top of the normal range). I may try and get blood tests for ACTH, cortisol etc. but I have seen people with PAS report normal values for these hormones. Despite this, the study seems to indicate that retinoic acid causes a dysregulation with the glucocorticoid receptor. Hence, this dysregulation could theoretically remain even if cortisol etc. has normalized.
3 Likes
good luck! keep us updated on your side effects and how its all going. btw… where/how would you obtain this?
2 Likes
My DHEA was also high, it was 600! Damn! Top range was 590 i think. That thread is still here.
Goodluck and keep us updated.
2 Likes
Yes this is interesting as I have noted others to have DHEA as well. I think @Dubya_B also had high DHEA in his blood tests.
2 Likes
Sorry this has been a very very long read and I have very long mentally exhausting workdays.
You’re hypothesizing that high progesterone levels (in the brain) are the likely reason for PFS/PAS? I’m just trying to draw a conclusion out of all the walls of text above.
1 Like
Hi there,
No problem, if you just read the first few paragraphs I have written a summary of the theory. But yes I think it is plausible that PAS is linked to persistently elevated levels of progesterone either during treatment which causes some form of dysfunction which needs to be corrected or these changes in progesterone production continue after stopping treatment and so remains a problem resulting in PAS.
This theory relates to more to PAS as the research is linked to metabolites of isotretinoin and progesterone. However I have seen a theory which links PFS to progesterone as I believe finasteride does have some progestagen activity but I haven’t spent much time looking into that yet.
1 Like
one pillers break this theory immediately. All hormones were measured thousands of times by majority of users, there is no single hormone that would indicate the cause of the PAS.
I haven’t heard of many one pillers who have full blown PAS but this in no way breaks a theory. Just reverting to one pillers can break this theory, on that logic one pillers could break every plausible theory. Can you think of a single theory which would make sense in the light of supposed one pillers? Does that mean all theories are not legit? There is certainly a theory which is correct and works in spite of one pillers.
I imagine one pillers who develop full blown PAS are very much an exception to the rule (a rarity), I am sure these individuals do exist but they are likely to have some kind of extreme sensitivity to the effects of PAS. They may have multiple gene variants, each of which makes them more sensitive to developing PAS than the average person. Thus the combination of these gene variants together makes these individuals hypersensitive, so that they develop full blown PAS very quickly. In this light, these individuals do not disprove this theory.
What if a person has multiple gene variants such as:
- A variant which greatly reduces the ability to eliminate Isotretinoin metabolites from the body.
- A variant which greatly increases progesterone receptor expression or binding capacity.
- A variant which greatly increases progesterone production in response to isotretinoin metabolites.
If you imagine all three of these in a single individual, it becomes possible for just a few pills to lead to PAS. Again though, these individuals would be very much rare cases and from what I have read, they do appear very rare as I haven’t heard of any, I have only heard of PFS people who took a single pill.
Again how do you explain why PAS can develop after a single pill in some people but it can also develop only in a second course of isotretinoin, meaning individuals take an entire course of isotretinoin but do not develop PAS.