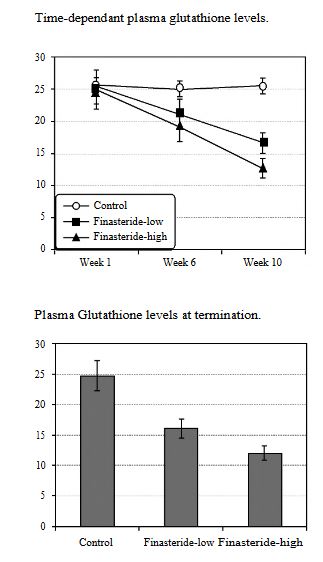
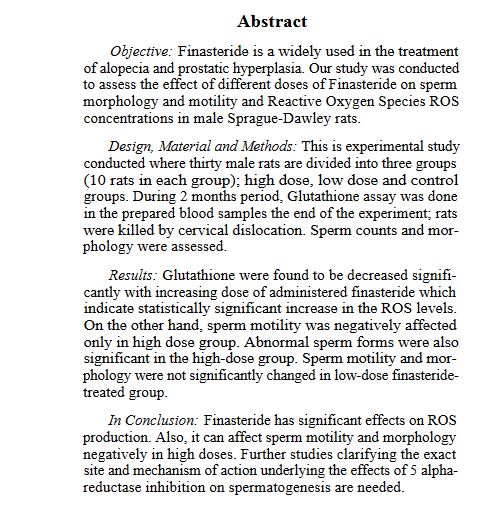
So it does seem that finasteride depletes glutathione. Depletion of glutathione seems to be a huge factor in the development of CFS like diseases.
medicaljournalofcairouniversity. … ber/30.pdf

So it does seem that finasteride depletes glutathione. Depletion of glutathione seems to be a huge factor in the development of CFS like diseases.
medicaljournalofcairouniversity. … ber/30.pdf
I took “l-glutathione reduced” 1-2 capsule (250mg) the last few nights and feel more in peace waking up in the morning which makes sense if it’s what protects your brain. Usually I feel shattered in the morning (since PFS began) with permanent tension and anxiety. I hope those who have daily headaches or feel on-edge or like their mind is old and losing braincells from stress try this and report back. I also noticed taking Tyrosine 1 capsule (500mg) gave me vivid dreams which I normally never get since the time PFS damaged my REM sleep.
If you are gong to raise glutathione I would be careful. I felt much worse after nebulizing glutathione. I also seem to feelworse when I take a product containing setra glutathione. It is common in CFS that people have bad reactions to glutathione. Possibly the glutathione is becoming oxidized and adding to the oxidative stress load. In CFS most try and raise it with other methods such as with herbs and methylation. Another guy here told me nebulizing glutathione helped him, so we may respond differently.
ncbi.nlm.nih.gov/pmc/articles/PMC19696/
This article shows that glutathione depletion leads to an imbalance in the immune system. The th2 arm of the immune system produces antibodies which bind to mast cells, eosinophils and others along with the antigen. Ufnortunatly this arm of the immune system is not very effective at dealing with some types of pathogens.
I have high eosinophils since PFS as mentioned and I assume my IgE went up when my eosinophils did. This is the classical th2 response of the immune system. A large percent of guys here have elevated immunoglobulins like me.
The below study is for animals.
Abstract
Current thinking attributes the balance between T helper 1 (Th1) and Th2 cytokine response patterns in immune responses to the nature of the antigen, the genetic composition of the host, and the cytokines involved in the early interaction between T cells and antigen-presenting cells. Here we introduce glutathione, a tripeptide that regulates intracellular redox and other aspects of cell physiology, as a key regulatory element in this process. By using three different methods to deplete glutathione from T cell receptor transgenic and conventional mice and studying in vivo and/or in vitro responses to three distinct antigens, we show that glutathione levels in antigen-presenting cells determine whether Th1 or Th2 response patterns predominate. These findings present new insights into immune response alterations in HIV and other diseases. Further, they potentially offer an explanation for the well known differences in immune responses in “Th1” and “Th2” mouse strains.
DISCUSSION
Studies presented here demonstrate that GSH levels in APC play a central role in determining whether Th1 or Th2 cytokine response patterns predominate in immune responses. Using two immunologic models and three methods to deplete GSH, we show that in all cases, GSH depletion leads to a shift away from the typical Th1 cytokine profile and toward Th2 response patterns.
This study shows the same thing happening in humans with HIV.
So I believe that this is much more likely the cause of PFS rather than any direct hormonal changes.
Finasteride depletes glutathione in those who are genetically or environmentally sensitive. Some dormant pathogens reactivate or one aquires a new pathogen. The body can not keep this pathogen undercontrol with depleted glutathione. The th2 arm of the immune system is engaged which suddenly causes massive symptoms of disease also known as “sickness behavior”. This inflammation causes dysregulation of the gut suddenly an then you are stuck in a vicious cycle. This is essentially one of the main theories of how CFS starts. I have already documented that we suffer the same symptoms of those with CFS.
So how to recover from this? Look at the existing recoveries, they match this kind of pattern, some get lucky and recover with time others do many things to try to boost their cellular health or gut health to stabilize their body.
ncbi.nlm.nih.gov/pubmed/26133750
Liposomal Glutathione Supplementation Restores TH1 Cytokine Response to Mycobacterium tuberculosis Infection in HIV-Infected Individuals.
Ly J1,2, Lagman M1,2, Saing T1, Singh MK1,2, Tudela EV1,2, Morris D2, Anderson J2, Daliva J2, Ochoa C3, Patel N3, Pearce D4, Venketaraman V1,2.
Author information
Abstract
Cytokines are signaling biomolecules that serve as key regulators of our immune system. CD4(+) T-cells can be grouped into 2 major categories based on their cytokine profile: T-helper 1 (TH1) subset and T-helper 2 (TH2) subset. Protective immunity against HIV infection requires TH1-directed CD4 T-cell responses, mediated by cytokines, such as interleukin-1β (IL-1β), IL-12, interferon-γ (IFN-γ), and tumor necrosis factor-α (TNF-α). Cytokines released by the TH1 subset of CD4 T-cells are considered important for mediating effective immune responses against intracellular pathogens such as Mycobacterium tuberculosis (M. tb). Oxidative stress and redox imbalance that occur during HIV infection often lead to inappropriate immune responses. Glutathione (GSH) is an antioxidant present in nearly all cells and is recognized for its function in maintaining redox homeostasis. Our laboratory previously reported that individuals with HIV infection have lower levels of GSH. In this study, we report a link between lower levels of GSH and dysregulation of TH1- and TH2-associated cytokines in the plasma samples of HIV-positive subjects. Furthermore, we demonstrate that supplementing individuals with HIV infection for 13 weeks with liposomal GSH (lGSH) resulted in a significant increase in the levels of TH1 cytokines, IL-1β, IL-12, IFN-γ, and TNF-α. lGSH supplementation in individuals with HIV infection also resulted in a substantial decrease in the levels of free radicals and immunosuppressive cytokines, IL-10 and TGF-β, relative to those in a placebo-controlled cohort. Finally, we determined the effects of lGSH supplementation in improving the functions of immune cells to control M. tb infection by conducting in vitro assays using peripheral blood mononuclear cells collected from HIV-positive individuals at post-GSH supplementation. Our studies establish a correlation between low levels of GSH and increased susceptibility to M. tb infection through TH2-directed response, which may be relieved with lGSH supplementation enhancing the TH1 response.
ncbi.nlm.nih.gov/pubmed/16598818
Endocrine disruptors that deplete glutathione levels in APC promote Th2 polarization in mice leading to the exacerbation of airway inflammation.
Kato T1, Tada-Oikawa S, Takahashi K, Saito K, Wang L, Nishio A, Hakamada-Taguchi R, Kawanishi S, Kuribayashi K.
Author information
Abstract
Endocrine-disrupting chemicals (EDC) are ubiquitous in environment and may have various undesirable effects on human health. In the present study, we have shown that some EDC [benzophenone, p-octylphenol, and tributyltin chloride (TBT)] promoted strong Th2 polarization via suppression and augmentation of Th1 and Th2 development, respectively, from naive CD4+ T cells primed with anti-CD3 and splenic antigen-presenting cells (APC). The effect was indicated to be indirect via suppression of IL-12 production and augmentation of IL-10 production of APC, which are critical for the Th1 and Th2 development, respectively. Such modulation of cytokine production by EDC was associated with reduction of intracellular glutathione levels in APC. IL-10 deprivation or the addition of N-acetylcysteine, which replenishes intracellular glutathione level during priming, cancelled the effect of EDC on the promotion of Th2 polarization. Oral administration of TBT, which most effectively promoted Th2 polarization in vitro, exacerbated airway inflammation in a murine model of allergic asthma with concomitant enhancement of Th2-type immunity. Collectively these results suggest that EDC such as benzophenone, p-octylphenol, and TBT promote Th2 polarization indirectly via the depletion of glutathione in APC and subsequent modulation of IL-10 and IL-12 production that might result in the exacerbation of allergic diseases.
Glutathione redox regulates airway hyperresponsiveness and airway inflammation in mice.
Yoko Koike, Takeshi Hisada, +7 authors Kunio Dobashi
Glutathione is the major intracellular redox buffer. We have shown that glutathione redox status, which is the balance between intracellular reduced (GSH) and oxidized (GSSG) glutathione, in antigen-presenting cells (APC) regulates the helper T cell type 1 (Th1)/Th2 balance due to the production of IL-12. Bronchial asthma is a typical Th2 disease. Th2 cells and Th2 cytokines are characteristic of asthma and trigger off an inflammation. Accordingly, we studied the effects of the intracellular glutathione redox status on airway hyperresponsiveness (AHR) and allergen-induced airway inflammation in a mouse model of asthma. We used gamma-Glutamylcysteinylethyl ester (gamma-GCE), which is a membrane-permeating GSH precursor, to elevate the intracellular GSH level and GSH/GSSG ratio of mice. In vitro, gamma-GCE pretreatment of human monocytic THP-1 cells elevated the GSH/GSSG ratio and enhanced IL-12(p70) production induced by LPS. In the mouse asthma model, intraperitoneal injection of gamma-GCE elevated the GSH/GSSG ratio of lung tissue and reduced AHR. gamma-GCE reduced levels of IL-4, IL-5, IL-10, and the chemokines eotaxin and RANTES (regulated on activation, normal T cell expressed and secreted) in bronchoalveolar lavage fluid, whereas it enhanced the production of IL-12 and IFN-gamma. Histologically, gamma-GCE suppressed eosinophils infiltration. Interestingly, we also found that gamma-GCE directly inhibited chemokine-induced eosinophil chemotaxis without affecting eotaxin receptor chemokine receptor 3 (CCR3) expressions. Taken together, these findings suggest that changing glutathione redox balance, increase in GSH level, and the GSH/GSSG ratio by gamma-GCE, ameliorate bronchial asthma by altering the Th1/Th2 imbalance through IL-12 production from APC and suppressing chemokine production and eosinophil migration itself.
It is very interesting to not the high prevalence of a history of asthma in PFS guys. Asthma is said to be a th2 based disease in which the body releases immunoglubulins in responses to allergens. This could indicate we had a unbalanced immune system and fin was like a nuclear bomb for us by further skewing the immune system.
It might be that the crash occurs when the body has became so depleted by the drug the th2 arm of the immune system is activated causing sudden huge inflammation and feelings of sickness. Many people crashed when they had extra stress or took antibiotics.
INflamation causes sickness behavior, which includes loss of libido.
Man you have to confirm that the hypothesis is valid, before trying to heal it, we have to recollect some markers to know if we are in the situation before correcting it.
Good job pointing this out, inmune system is related as I havent had a flu since pfs, and I had flu every year since pfs.
I saw the top immunologist today about my elevated IgE and Eosinophils. First he thought it was fungus in the sinus but that was rulled out, then he said maybe a parasite so gave me albendazole, which did not help.
He has no more ideas, he doesnt know why my eosinophils were normal before fin and are now high. Very strange.
So what would be the goal here has far as treating based on this mechanism?
decreasing or increasing immune system ?
in my case my ige is elevated eosinophils are high. This is the th2 system. I beleieve i need to some how boost the th1 system to stop the th2 activation.
My glutathione is deplete so is that the cause of elevated th2? Maybe, what is depleting glutathione? infections? environment? toxin accumulation? Disbiosis? hormones?
My organic acid testing showed elevated d-lactate, stool testing showed high enteroccus and strep. So dysbiosis is a large factor in this but I am not sure the cause or how it relates to the high eosinophils and IgE.
Another guy who recovered and relapsed
solvepfs.com/viewtopic.php?f … ilit=aztec
Many have theories of complicated damage to enzymes, brain or endocrine system, I am very interested to hear how they explain all these cases of people recovering then relapsing years later? I am all ears for an explanation. To me this phenomenon seems to rule out any of these complex theories. In my opinion it is more like the immune system is trying to keep something at bay, once the body gets stressed these people relapse.
Been taking lipsomal glutathione for about 1 week, think i feel worse after taking it.
Nebulized glutathione made me feel a lot worse.
I have some pill form mixed with herbs and that seems to make me worse.
Not sure what to think about that.
This photo looks faded out a bit. But there has been a red rash on my foot for many months. Maybe I noticed it 6 months ago.
It gets redder when I feel worse. Today i feel so tired to walk and it is much redded. Sometimes it is almost not visable. Always in the exact same spot. Top of left foot.
I think it is connected to my high eosinophils since taking fin. I have no idea what my eosinophils are fighting?
Dihydrotestosterone Stimulates Cerebrovascular Inflammation through NFκB, Modulating Contractile Function
ncbi.nlm.nih.gov/pmc/articles/PMC2658637/
In my opinion, our body react to DHT after we quick Finasterie, our system was adapted a low levels of inflammation.
I got more articles related to this, I will collect it and I will posted back, cos in my opinion high inflammation market is a red flag to our symptoms, even I read that Lipopolysaccharide LPS ans TNF-alpha silent 5AR2 gene. and inhibitors of LPS and TNF-alpha activated it.
I crashed while on like many.