
Looking at the reference range of the allopregnanolone on ZRT labs LCMS salvia hormone test we can see that the reference range is as follows:
LESS then 15 pg/mL
So when I first seen this I was confused. So I emailed the owner of ZRT lab and he explained it to me. When a lab uses a reference of “Less then 15 pg/mL” they are saying that anything less then 15 pg/ml is normal and anything over 15 pg/mL is high. This type of a reference range is only telling you if your value is high.
In this case because my allopregnenolone was not high it’s considered normal as far as this reference range is concerned. However it’s not actually telling me what my allopregnenlone level is. It’s just telling me that it’s not high. The doctor/researcher/scientist who owns ZRT lab explained that in certain instances when patients go on Finasteride their allopregnenolone can go high which can make someone feel shitty so this test to an extent can be used to monitor patients while on Finasteride. But like I said this tests is not telling me if I am producing low amounts of allopregnenolone or not. It’s just telling me that I do not produce high amounts of allopregnenolone.
Ok so now based on this test I know that I don’t produce high amounts of allopregnenolone. But I am still left thinking “do I produce low amounts of allopregnenolone”?
So the reason why I actually got ZRT’s urine hormone metabolite test was to see if I was low in allopregnenolone or not. Again I knew that I was not producing high amounts of allopregnenolone from ZRT’s LCMS salvia test but I still did not know if I was producing low amounts of allopregnenolone. So I got the urine test knowing that ZRT’s urine hormone metabolite test (the one that you ordered) would not only tell me if I was producing low amounts of allopregnenolone but that it would also tell me exactly what my urine allopregnenolone levels are. Why? Because ZRT’s labs urine hormone metabolite test has a full reference range for the urine allopregnenolone value. It’s not just saying “less then such and such is normal” because it’s not high. It’s actually providing a normal reference range like we are use to seeing in our blood hormone labs.
So now I get my urine hormone metabolite allopregnenolone results back and see that I am peeing out top of the reference range level allopregnenolone levels….
Obviously common sense makes me ask my self this question:
If I know I am not producing high amounts of allopregnenolone per the saliva test THEN WHY AM I PEEING OUT HIGH AMOUNTS OF ALLOPREGNENOLONE???
I’m either producing normal or low amounts of allopregnenolone and I am peeing out most of it? Well why? If I was producing high amounts of allopregnenolone I would suspect to see high amounts of in my urine. Produce more in my mind means pee out more. But I am peeing out more in spite of not producing high amounts of it. This is what catches me eye. Get my logic?
To answer the rest of the questions:
Progesterone converts to 5a-DHP via the 5AR enzyme. Then 5a-DHP converts to allopregnenolone via the 3a-HSD enzyme.
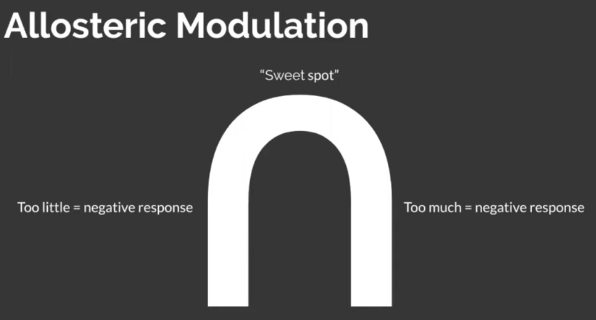
Obviously I understand that a lot is unknown about allopregnenolone and the implications with messing with it. Which is why there should not be a drug that messes with it without the impact of messing with it having been properly studied. They do know that allopregnenolone is a positive allosteric modulator of the GABA receptors. My understanding of what this means is that not only is allopregnenolone agonizing the GABA receptors but it “modulates” them. In my mind this means that allopregnenolone is making sure there is enough action on the GABA receptors adjusting their sensitivity in a way that allows them to respond “positively” to GABA. Opposed to pregnenolone sulfate which is negatively modulating the GABA receptors hindering the GABA receptors response to GABA. It’s also my understanding that the GABA receptors need a proper balance of positive and negative modulation to work properly. The GABA receptors should not be too sensitive but they should not be too insensitive. Which is why I am assuming “mother nature” gave us neurosteriods that both positively and negatively modulate the GABA neurotransmitter receptors. So this is why I am theorizing that I have a GABA receptor imbalance. Because I do not appear to be producing enough pregnenolone sulfate while I am peeing out top of the reference range amounts of allopregnenolone. This to me suggests too little negative modulation of the GABA receptors which may be why my body is peeing out as much allopregnenolone as possible in order to avoid too much positive modulation in lack of negative modulation. If you read about what can happen when the GABA receptors are not balanced things go bad. Like seizures and all kinds of horrible things. So maybe my body is smart enough to stop as much positive modulation of the GABA receptors as possible by getting rid of it’s allopregnenolone in the urine knowing what the outcome will be if the allopregnenolone hits the GABA receptors with not enough negative modulation (pregnenolone sulfate)
Disclaimer:
This is all theory based on my own labs. So I am not claiming to know what PFS is. I am simply trying to explore my theory further in others

 is that for real?
is that for real?