You are lucky you have a doc willing to work with you to investigate this further… hopefully you guys might turn up some answers…
This is just a theory, but I’m not sure if it holds any water since I and others DID RECOVER when we quit the drug – approximately 1.5-2 weeks after stopping, as DHT returned… however, recovery was short-lived and within 1-2 weeks of initial recovery, things starting going downhill fast (drop in T levels, shrinkage, loss of libido etc).
Plus the fact I experienced a semi-recovery 1 year later when I had Norwalk virus for 2 days and my penis and testes returned to former size, along with decent libido, tells me this is not permanent and likely not a mutation.
HOWEVER – if you still want to investigate the mutation route further, I can’t say I’ve come across any studies that directly relate Finasteride as causing a mutation in 5AR-II… however, these may be of general interest (note some relate to prostate cancer, however, thus may not be relevant):
books.google.com/books?hl=en&lr= … gsZAvVuuWM
(see pages 45 - 62 for general info on AR function/mutations)
propeciahelp.com/forum/viewt … t=mutation (note Fin also downregulates AR)
propeciahelp.com/forum/viewt … t=mutation
propeciahelp.com/forum/viewt … t=mutation
"Another cause of isolated secondary hypogonadism is a mutation of the GnRH receptor. In these cases, GnRH is secreted by the hypothalamus but does not stimulate LH secretion by the pituitary. A third cause is a mutation of the DAX-1 gene, which leads to hypogonadotropic hypogonadism and to adrenal hypoplasia congenita. "
clincancerres.aacrjournals.org/c … /5/11/3578
“We found one tumor from a finasteride-treated patient with a mutation in the steroid binding domain at codon 726 leading to an Arg-to-Leu substitution. This mutation was also present in the germ-line DNA of this patient.”
"Taken together, we have shown here by CGH that prostate cancers appearing during finasteride treatment have only few genetic alterations and that, in some cases, alterations in the AR gene may be involved in the adaptation of the DHT-deficient milieu. Further studies are also needed to demonstrate the importance of Arg726Leu germ-line mutation of the AR gene in the etiology of prostate cancer and especially finasteride-associated prostate cancer among Finnish and other populations. "
pubmedcentral.nih.gov/articl … tid=544619
“Given that hormone ablation selects for AR mutations and these mutations can cause the development of aggressive and metastatic disease, it could be argued that maintaining an intact androgen signaling axis would be of benefit to most patients”
jcem.endojournals.org/cgi/reprint/80/7/2149
(has info on amino acid substitutions and other changes in 5AR2 due to mutation)
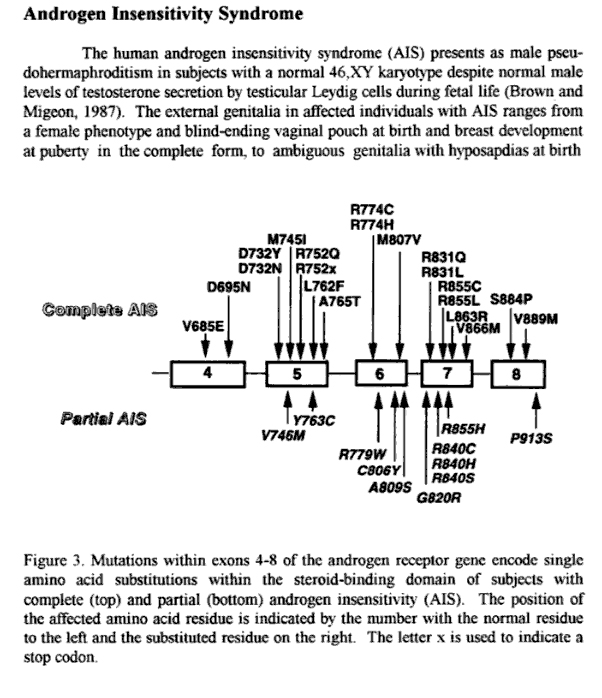
Your situation is a bit different than others here in that you were already on TRT when you took Finasteride, which may have impacted things too. Not sure how though… anyway, as for Androgen Resistance, have you investigated Androgen Resistance/Insensitivity Syndrome?
en.wikipedia.org/wiki/Androgen_i … y_syndrome
emedicine.com/ped/topic2222.htm
Note the lab tests and treatment options in the above link!
Also here is a potential genetic test for mutations in AIS: jcem.endojournals.org/cgi/conten … /88/5/2185
"Five mutations in the ligand-binding domain (LBD) of the human androgen receptor (hAR) found in patients with varying degrees of androgen insensitivity syndrome (AIS) were investigated for their effects on receptor dynamics. "
Question: What was the result of the genetic screen (CAG repeats)? Did it come back normal? I assume so since he is now interested in testing at the enzyme/genetic level.
Besides trying to test at the cellular level (by testing genital skin fibroblasts for 5AR2 enzymatic activity, or genetic PCR analysis of 5AR2 gene to check for mutation), suggest you test for the various hormones/ratios listed in this thread (my post, 11th down, with the screenshot), since that is also something Finasteride can throw out of whack (and is related to liver C19/C21 metabolism):
propeciahelp.com/forum/viewtopic.php?t=1079
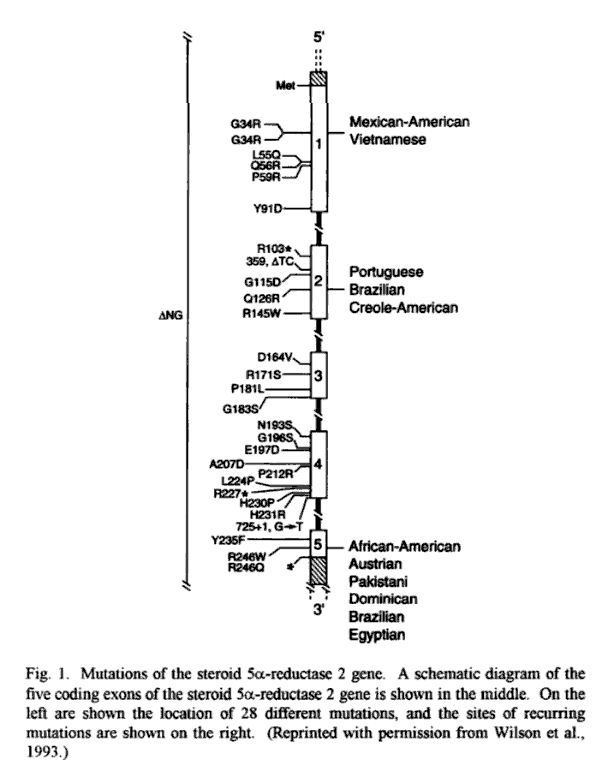
Also, consider testing 5AR2 deficiency as follows, from “Molecular Study of the 5 a-Reductase Type 2 Gene in Three European Families with 5 a-Reductase Deficiency”
jcem.endojournals.org/cgi/reprint/80/7/2149
“Diagnosis should be determined on the basis of physical examination, pedigree analysis, analysis of basal and post-hCG-stimulation plasma T and DHT levels, 5/3/5,
urinary steroid metabolite ratio, and in some cases by measurement of 5aR activity in cultured genital skin fibroblasts (13,14). However, as in family 1, enzymatic activity is sometimes within the normal range (6, 15). Isolation and sequencing of the complementary DNA encoding 5aR2 (5) provides the molecular tools required for definition of the gene abnormalities responsible for 5aR deficiency.”
You might also want to investigate 17b-Hydroxysteroid Dehydrogenase 3 Deficiency?
rarediseasesnetwork.epi.usf.edu/ … x.htm#nomo
“Plasma androstenedione levels are elevated 10-fold or more, whereas testosterone and dihydrotestosterone levels are in the low or low normal range for normal males”
captura.uchile.cl/dspace/bitstre … /Rey_R.pdf
“The association of a lack of testosterone increase after the hCG test and a testosterone/4-A ratio less than 0.5 was considered as highly predictive of 17-HSD deficiency (25). Finally, the activity of 5a-reductase was evaluated by using the testosterone/DHT ratio after hCG stimulation. A testosterone/DHT ratio higher than 35 was considered as highly predictive of 5a-reductase deficiency (26). A testosterone hCG/basal ratio of at least 2 associated with AMH SDS of at least 2 was considered as highly predictive of partial androgen insensitivity.”
Regarding liver involvement – you might want to get this investigated further… the liver plays a huge role in steroidogenesis and thus, some theorize Finasteride has affected liver steroidogenesis/metabolism, especially considering that 5AR is produced there (see study in below link) and because Finasteride is heavily metabolized by Cytochrome P450 system/CYP3A4 enzymes (and inhibits hepatic C19/C21 metabolism as well, plus 5AR is found in liver), that this may have caused post-Fin issues:
propeciahelp.com/forum/viewtopic.php?t=789
Also note that elevated liver enzymes can occur as a result of Fin use:
propeciahelp.com/forum/viewtopic.php?t=182
propeciahelp.com/forum/viewtopic.php?t=1024
propeciahelp.com/forum/viewtopic.php?t=1023
Some other general thoughts about how we came to this state (proposed by Galapagos and myself): propeciahelp.com/forum/viewt … t=mutation
As for finding a lab – try Quest Diagnostics, they have a location in the UK but may have in Switzerland (call and see): questdiagnostics.com/brand/c … ities.html
Also this lab, don’t know how legit they are but they are in the UK: sas-centre.org/home.html
Beyond that, your doc might consider contacting University medical research departments or Hospitals as a potential testing facility. Or, contact the authors of studies where you see the tests being done – they are obviously possible to get done, somewhere.
Keep us posted.