Cortisol could be high or normal, but the issue is not cortisol or GC in my opinion. Those have not been affected as, IMO, they are not part of the main 5ar complex fin attacked.
3a-HSD neutralizes DHT. If DHT went lower because of 5ari, I believe the body had to lower 3a-HSD to try and maintain some DHT.
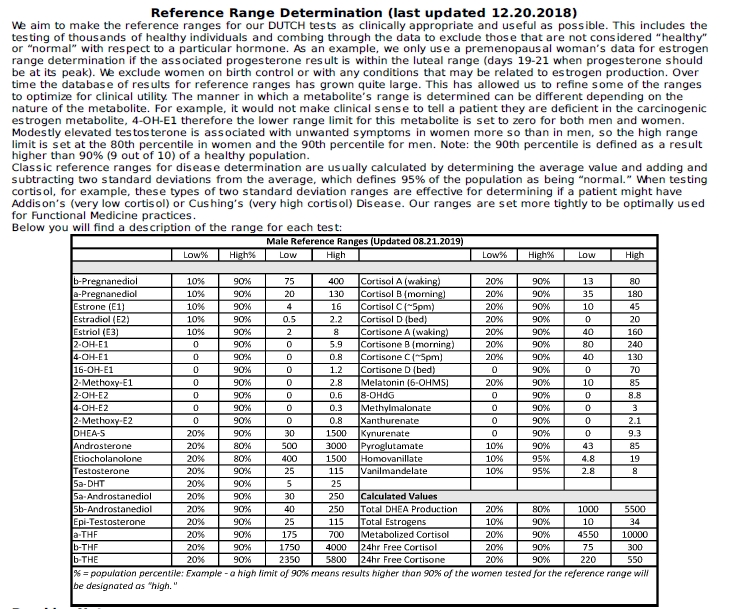
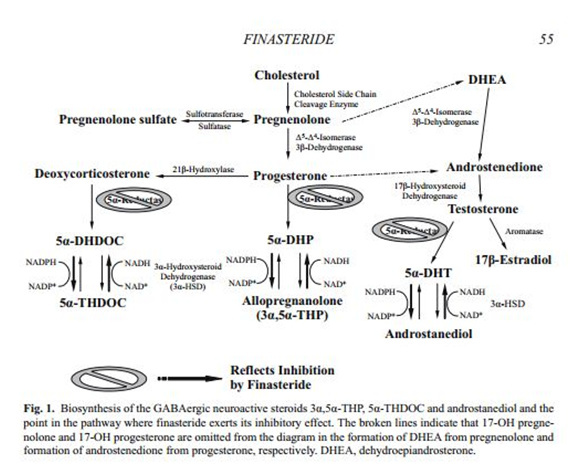
If you’re to test stuff, test progesterone (should be 0.8ng/ml) and you can either test 3b and 3a-HSD, or their metabolite 5a-DHP and Allopregnanolone as the metabolite is more exactly what you want and they indicate if the precursors are working correctly.
If you don’t mind, tell me your results !
ZRTLab.com can do those. If you do it with them, please tell me how much they charge !
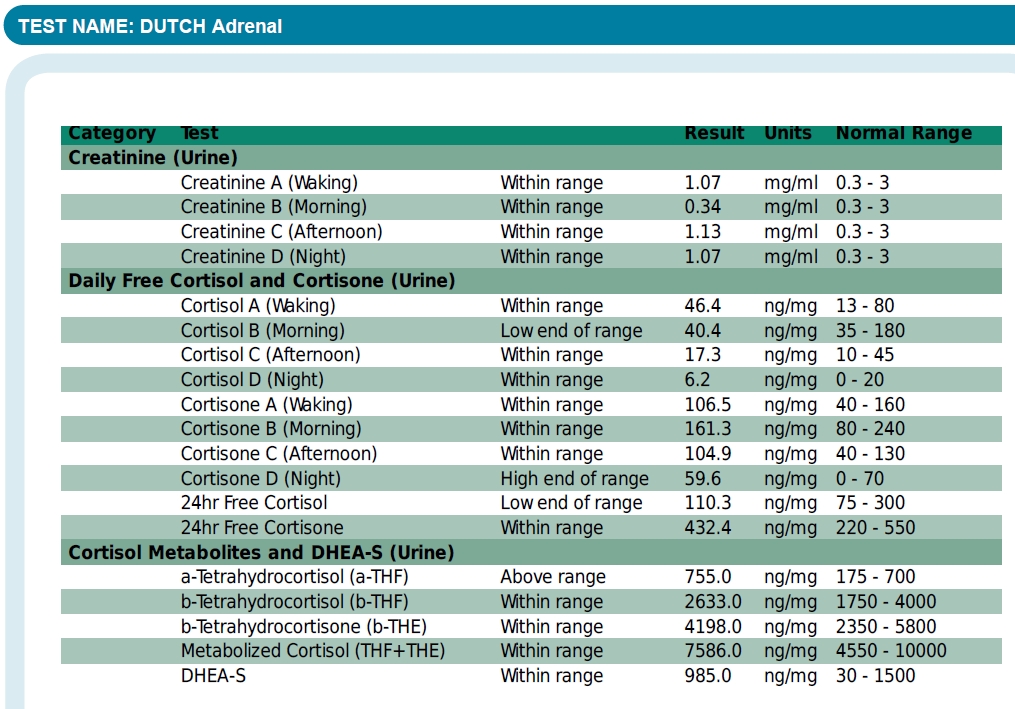
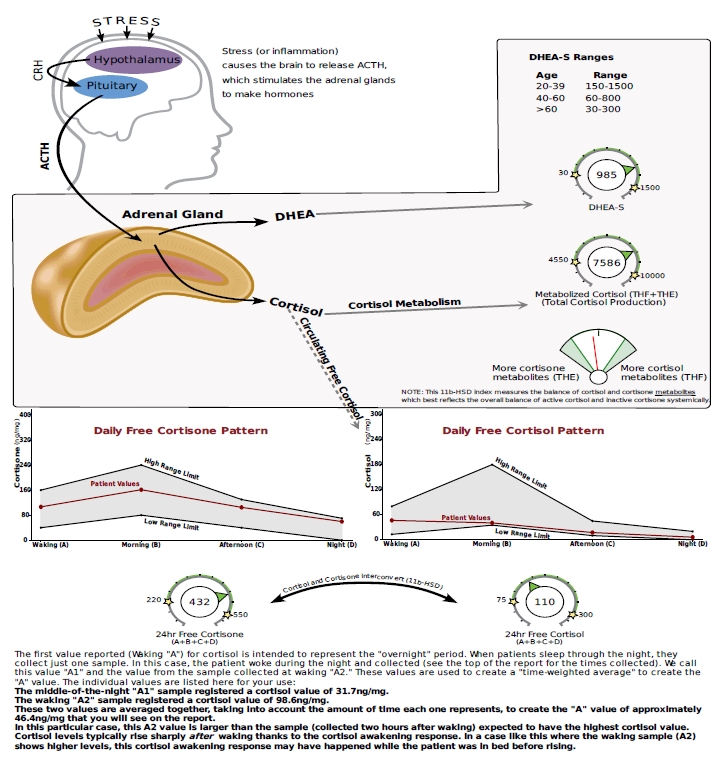
I agree with everything you said. The fact that my recent cortisol and cortisone results show that I have proper amounts of active cortisol converting to inactive cortisone confirms that my 11-Beta-Hydroxy Steroid dehydrogenase (11B-HSD) enzymes are working properly. This is important to confirm because your active cortisol could be in proper amounts in plasma but if not enough of it is converting to inactive cortisone this could result in too much cortisol binding to the mineral corticoid receptors brining on similar symptoms that we experience. So ruling this out is good and I did rule this out.
My recent PROGESTERONE tested in @: <0.5 <1.4 ng/mL
So my recent 0.5 Progesterone result is close to your 0.8 Mark. This suggests that my 3B-HSD enzymes are working properly. However, my 3B-Androstanediol (3B-diol) tested in @ below lab reference range low in 2013. Low 3B-diol suggests that my 3B-HSD enzymes are not working correctly because 3B-HSD also converts DHT to 3B-diol. BUT additionally 17B-hydroxysteriod dehydrogenases (17B-HSD) also convert’s DHEA to 3B-diol. So with this being said my low 3B-diol readings may be in result of 17B-hydroxysteriod dehydrogenases (17B-HSD) not working correctly, which, is suggested by the fact that it appears 3B-HSD, is able to convert proper amounts of Pregnenenolone to Progesterone via 3B-HSD.
There is also the possibility that 5AR recovered enough or was not effected enough in certain places to be able to convert proper over all amounts of T-DHT but not in other places where conversion of progesterone into 5a-DHP takes place. Following this logic there is also a possibility that 3a-HSD could be working well enough in certain areas to be able to covert DHT to 3a-diol but not well enough to convert 5a-DHP into Allopregnanolone. Also enzymes such as 3a-Hydroxysteriod dehydrogenase (3a-HSD) can also convert 3a-diol back into DHT and compensate by doing just this when 5AR is no longer working properly. So after really digging into this it becomes clear that the only way for each individual to know their status on each one of these parameters is to get tested for everyone one of them or as many of them as possible including 5a-DHP and Allopregnanolone like you said.
I am looking into as many labs and companies as possible to try to find the best place to have these tested at the best price. I will let you know.
This is all interesting and something I’ve also tried to figure out in the past few moths. Here is my recent 24h Cortisol test results for comparing. This was done trough Dutch Adrenal test which was measured from urine, my former test was done trough saliva ->
So basicly my 24h Cortisone curve is quite optimal and its making the spike on the mornings but the conversion to Cortisol doesnt work at all. The morning spike is lacking and Cortisol is very low overall througout the day.
There is no more reason to question ZRT’s accuracy compared to quest diagnostics or lab corp.
The issue with ZRT is that they refuse to sell the LCMS saliva test kit directly to us. They want us to go through providers that they have partnerships with and request through their providers to order us the kit. The bad thing about this is now we need to deal with money hungry functional health doctors that want to scam us and charge us “to go over the results with us” who know less about allopregnanolone than we do
We just need to be able to buy the kit directly from ZRT labs. I suggest that you call and ask them if you can buy their LCMS saliva test and refuse to go through their “linked” providers to get the test. Show them that there is a demand for their LCMS saliva test kit but that we want to buy it directly from them like they sell many of their kits directly to individuals. The point to get across to ZRT is that we have already been through enough nonsense so the last thing we want to deal with is one of their providers who want us to pay out of pocket for “their medical services”.
I am getting ZRT labs LCMS Saliva steroid profile kit done. It will test for allopregnanolone. The problem is that ZRT labs requires you to go through one of their providers to order the LCMS Saliva steroid profile kit which is undesirable. They are functional health doctors who get the LCMS test kit from ZRT for cheep and price gouge us. The provider that i got mine through made $300 plus off the sale of one kit to me and wants to charge me more to “let me have my results”
ZRT’s concern is that if they sell us the LCMS kit directly they will feel obligated to help us. I attempted to explain to them that people in this community have already been let down by the medical establishment so the last thing we are going to do is call ZRT for “help”
Learn more about which metabolites/neurosteroids were or were not affected
Learn more about whether or not different metabolites are affected differently in different PFS victims. You could be low in ALLO and or THDOC and I may not be
Having the opportunity to narrow in on what has been affected in my case. In 2013 I was low in 3b-diol. So having had the opportunity to learn that 3b-diol acts as a potent agonist of the estrogen receptor allows me to possibly make a connection with the fact that I also get worse from taking an estrogen Aromatase inhibitor. This can help me explore a possible path to recover. Maybe I’m deprived of estrogen which would certainly be something that I would have never have considered if I did not know that at least at one time I was low in 3b-diol. Maybe even figuring out that being low in 3b-diol may be a sign that you are a PFS vicim who will get worse from taking an aromatase inhibitor. This forum had a guy once who killed him self after taking an aromatase inhibitor while others get some results or at least not worse from taking an aromatase inhibitor. So potentially having a "maker’ to go by to know if you are someone who should or should not take an aromatase inhibitor would be helpful to say the least.
Taking metabolites/neurosteroids that we are personally low in and researching which enzymes are responsible for metabolizing it providing a clue as to which enzymes were affected. Researching if that enzyme uses the same co factor that Fin, Dut and possibly Saw P binds in order to see if this is a path that leads to anything
Supplementing what we are low in. If I am low in ALLO I am going to do what ever I need to do to get my hands on ALLO and take it. I will not assume that because
5a-DHP which concerts to ALLO did not cure me that taking ALLO would not cure me. But I’m certainly not going to go through what ever trouble that I would need to go through to obtain ALLO and take it if I don’t even know if I am low in it.
If I am low in THDOC I’m going to use every resource available to me to research THODC and the possible implications with not having enough of it.
Use the results to create awareness. Bring the results to my doctor’s attention to further the cause of this forum
Give the results to a lawyer to help initiate a case
In other words, anything I can do with the results will be my actionable response
years of pain and suffering to include punitive damages. Propeica lawsuits are difficult mainly due to the lack of explanation. Once a big find is made this will change.
I am getting my results no worries here and i’m not paying for them. It’s just the annoyance of needing to go through a doctor to have the test who’s first priority is money and to even need to remind them of my entitlement to my results . Access to the test without needing to deal with this BS would be much better
I posted that 3 years ago.It turns out 5ar transform some T into DHT. 3a-HSD eliminates DHT so that it doesn’t accumulate. They are not antagonists, but one makes DHT and the other destroys it to keep the balance.
I’m passed posting long theories, but if 5ar got much lower because of fin, 3a-HSD would also have to get lower IMHO in order to not eliminate all DHT in the body. This way, someone could produce less 5ar, less DHT but by having less 3a-HSD to eliminate the DHT, DHT could be at normal level.
However, low 5ar and low 3a-HSD still means low Allopregnanolone and low 5a-THDOC.
Very stressful, always hyped and anxious and having insomnia.
Hi Ozeph i’ve read this thread about 3a-HSD. I didn’t take Fin or any meds but only small doses of sulforaphane for a few days which has caused immediate insomnia (0-2 hours sleep per night for weeks) from the first days and still persistent after 5 month. I was already sleeping bad all my life and was used to being very sensitive when it comes to supplements and sleep but usually bad sideffects only lasted for a few days or a week.
It’s also my only real symptom. The other ones (if there are any they are very minor or caused by sleep deprivation).
The classic things like working out or taking cold showers make it worse (i think due to some cfs/pem related things i already had before) so they are not a solution.
What is your current state on this matter how to tackle it within the 3a/b-HSD?
Would it be worth a try to decrease 3a-HSD (how) while also decreasing 3b-HSD and increasing DHT with Tribulus or Creatine and supplementing something like pregnenolon?