
I just want to share my belief and research that led me there.
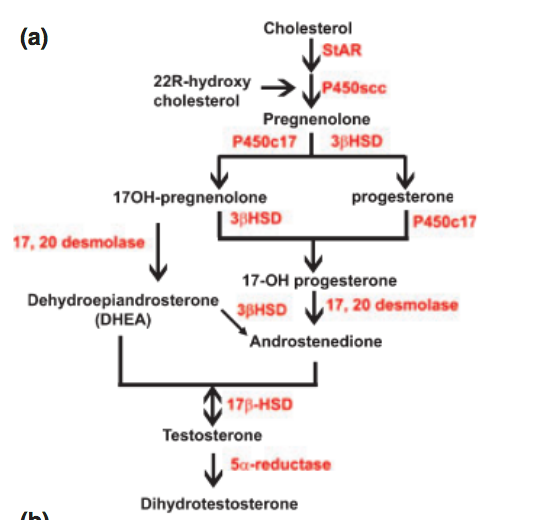
As I originally stated, I believed blocking 5aR lead to more downstream hormones being blocked. In other words, we blocked more than testosterone to dht, as I’ve been saying regarding allopregnanolone Here’s a pic of the precursors:

If you want to see the whole picture, this likely isn’t news to many:
https://upload.wikimedia.org/wikipedia/commons/1/13/Steroidogenesis.svg
Here’s a quick study on LH for progesterone creation:
“Luteinizing Hormone (LH)/human chorionic gonadotropin (hCG) stimulates progesterone biosynthesis in the corpus luteum by activating cAMP /protein kinase A (PKA) cascade"
Additionally, during my research and recovery, someone pointed out that HCG’s effect on StAR is valuable too:
“Stimulation of mLTC-1 mouse Leydig tumor cells with hCG resulted in the coordinate regulation of StAR mRNA expression and progesterone accumulation in a time-response manner"
Below is a picture of StAR’s importance in this hormone cascade. So it’s very likely a combo of StAR, Progesterone Synthesis & 5AR from HCG that resulted in my recovery.
A repost of HCG’s effect on 5AR:
Many times, searches of HCG leads to cycles in a steroid PCT setting with very high dosages to restart testosterone production. I believe that shouldn’t be conflated with the use of a low dose HCG protocol where I was aiming to restore neurosteroids, with sex hormones like testosterone and dht being a side effect. It’s common that PFS sufferers bloodwork show normal DHT so hypogonadism isn’t the issue here. In other words, this isn’t an HPTA restart. It’s the downstream hormones as the pictures show and the studies show HCG’s effectiveness.
I’m not a doctor and I’m just sharing what I researched and found helped me. I believe there’s an efficacious range of low dose hcg but I still say find a doctor that’ll work with you. I will edit anything the mods feel is against the rules.
