In my opinion it will take some real digging to figure out more about why some get better on HCG and why some get worse
Maybe before, during and after neurosteriod testing would tell us more. Get baseline levels, run HCG per Joe’s protocol wait until you feel better or worse and then run the same labs again while still on the HCG to see what changed. It would be expansive but worth it
I speak to @NewYorker often via phone. He is a great guy. I can tell you for a fact he is being 1000% honest with all of you and under the care of one of the best endocrinologists in Manhattan. He’s a very nice good dude. Don’t doubt his experiences he is being honest and truthful.
Looks like that downswing I had was just caused by stress, slept well last night and feel great cognitively. HCG wins for now
Just need ED to f**k off now. I went onto tinder not sure if good or bad thing since I prob wouldn’t be able to get up. Within 5 mins got insanely hot girls messaging me, I immediately logged off and now need solutions ASAP.
Viagra, Cialis, alpha blocker, penis injection, some sort of corticosteroid people here keep talking about?
Please please anyone with performance enhancement experience can you give to advice
I just want to share my belief and research that led me there.
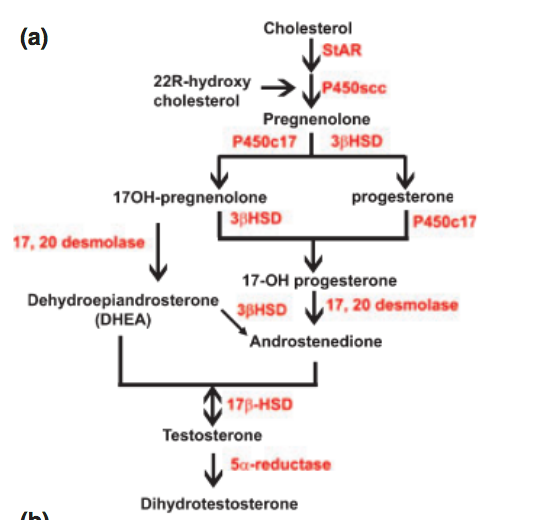
As I originally stated, I believed blocking 5aR lead to more downstream hormones being blocked. In other words, we blocked more than testosterone to dht, as I’ve been saying regarding allopregnanolone Here’s a pic of the precursors:
If you want to see the whole picture, this likely isn’t news to many:
Here’s a quick study on LH for progesterone creation:
“Luteinizing Hormone (LH)/human chorionic gonadotropin (hCG) stimulates progesterone biosynthesis in the corpus luteum by activating cAMP /protein kinase A (PKA) cascade"
Additionally, during my research and recovery, someone pointed out that HCG’s effect on StAR is valuable too:
“Stimulation of mLTC-1 mouse Leydig tumor cells with hCG resulted in the coordinate regulation of StAR mRNA expression and progesterone accumulation in a time-response manner"
Below is a picture of StAR’s importance in this hormone cascade. So it’s very likely a combo of StAR, Progesterone Synthesis & 5AR from HCG that resulted in my recovery.
Many times, searches of HCG leads to cycles in a steroid PCT setting with very high dosages to restart testosterone production. I believe that shouldn’t be conflated with the use of a low dose HCG protocol where I was aiming to restore neurosteroids, with sex hormones like testosterone and dht being a side effect. It’s common that PFS sufferers bloodwork show normal DHT so hypogonadism isn’t the issue here. In other words, this isn’t an HPTA restart. It’s the downstream hormones as the pictures show and the studies show HCG’s effectiveness.
I’m not a doctor and I’m just sharing what I researched and found helped me. I believe there’s an efficacious range of low dose hcg but I still say find a doctor that’ll work with you. I will edit anything the mods feel is against the rules.
Though HCG is an LH mimetic, it’s not LH. There appears to be extra benefits to hcg over LH. That’s an important distinction that even I’ve been known to use interchangeably.
I think high dose actually overwhelms neurosteroid receptors as well as over does it on the sex hormones. Even at this low dose, some ppl are experiencing high estrogen levels.
So are you telling me that the fact that my plasma 3b-diol is low and my urine allopregnenolone is high is not important?
Before assuming you are right consider this:
3b-diol is a potent estrogen receptor beta agonist. I get worse when I inhibit estrogen. I get better when I increase estrogen. Even though you are correct that my plasma 3b-diol levels are probably not going to match up with my 3b-diol CNS levels. But that does not mean my plasma 3b-diol levels are not important. Low plasma 3b-diol levels tells me that my 3b-HSD enzyme is converting low amounts of DHT into 3b-diol. Otherwise I would have higher amounts of 3b-diol in my blood if my 3b-HSD enzyme was converting higher amounts of DHT into 3b-diol. So low plasma 3b-diol levels is giving me a clue as to the status of my 3b-HSD activity.
Here is another example:
I don’t know my CNS allopregnenolone levels. But I do know that melcangi’s PFS study found low allopregnenolone in the CNS of the PFS group. I also know that my urine allopregnenolone is high. So based on this information I can make an educated guess that maybe allopregnenolone is low in my CNS as well because I’m getting rid of high amounts of Allopregnenolone in my urine which is excretory.
Maybe my body is excreting high amounts of allopregnenolone because it needs to get rid of it for a reason possibly pointing to an issue with the GABAa receptors in the brain. Because allopregnenolone in the CNS is a positive allosteric modulator of the GABAa receptor. So If there is too much action on the GABAa receptors body may be peeing out as much Allopregnenolone as possible so that the allopregnenolone does not make it to the GABAa receptors. Additionally my plasma
3a-diol is low and my urine 3a-diol is high. My DHT is not even converting to 3a-diol in high amounts in spite of my body peeing out high amounts of 3a-diol. This tells me that my body also wants to get rid of high amounts of 3a-diol which is also a potent GABAa receptor positive
allosteric modulator.
My point is that you are thinking one dimensionally and can’t make the same educated guesses I can because you don’t know your urine allopregnenolone levels or your blood 3a-diol or 3b-diol levels. I understand that you read somewhere else on this forum “that only CNS levels are relevant” but someone else posted that who also thinks one dimensionally. I’m working on that 4th dimensional level thinking. Humans will likely never see the 4th dimension but I’m certainly not going backwards…
seems like HCG can downregulate AR, but thats in female mice.
To gain an insight into potential roles of AR in this tissue, we demonstrated that eCG treatment increased AR expression in a time-dependent manner and subsequent treatment with hCG decreased AR expression in mouse fallopian tubes
Hello, and sorry for the delay in responding. I should be finishing the hCG injections in a couple of weeks. Overall, improvements are in the same areas I listed before, but still no real feelings of desire. I have a series of labs I’ll be organizing and posting, with the main improvement being testosterone numbers increasing substantially. I did feel the improvement for a few weeks, but I either got used to it, or it wore off. This pfs rollercoaster ride seems never ending.
I am under the guidance of an endocrinologist, and am meeting with him again March 6th. I’ll have another lab before meeting, and will include that and more detail soon.