
How can you account for the fact that PFS sufferers with T levels in range still saw benefit from TRT treatment?
Haven’t seen a single reliable account of enduring benefit. Across 15 years and tens of thousands of people. Anyway, you aren’t even doing it yourself but rather just sitting on Internet forum talking about it so this is too silly.
I spent considerable time creating a spreadsheet with accounts of successes. Please take the time to look at it before drawing invalid conclusions.
My doctor also prescribed me TRT and I’m not sure if to give it a try or not. My blood results shown that my LH is 2.2 (2-10), Testosteron 26.2 (>12), free Testo. 601 (>250), DHT 0.49 (0.50-2.00). Testo and free Testo seems to be in range. You know if a TRT would also increase my LH and DHT ?
2 Likes
Your doctor is either an idiot, or he is experimenting on you with TRT. You have 750 ng/dl of TT if that was written in Nmol/L. He may also a smart guy who thought about AR’s and that’s why he recommended TRT to you.
However, don’t listen their dosages and protocols. When it comes to dosages, nearly all doctors are severely faulty. This is proven here by many people.
Join T Nation or any other bodybuilding forums and ask a ‘‘safe but effective’’ dosage and duration.
No. It will reduce your LH. Why do you think people take HCG with TRT? It will increase DHT via increase on T.
Your issue is not hormonal man. It is your Androgen receptors and neurosteroids and modified SRD5A2 gene.
We don’t have the gene altering technology accessible now. I am sure some elitists already developed this technology and using it, CRISPR.
However, luckily with hormonal therapies, that epigenetic change also reverses back to normal as we can see from the recovered victims.
How to fix:
-Downregulate your upregulated AR’s.= Androgen HRT protocols.
-Supplement your neurosteroids.= HCG, Progesterone or spesific neurosteroid supplements if you have one lack on your blood tests. Pregnenolone etc.
-Pray
Man, i wish i had PFS instead of PAS. There is no good research done on PAS… But i have finally find a way for that too.
Anyways, in this case, don’t even wait, go for the TRT. To downregulate your AR’s. And add 250iu 3x a week HCG to it. Your LH on paper will become 0, but don’t worry it will recover, i experienced it by first hand.
Take HDAC inhibitors also and simple vitamins, Vit D, but nothing more fancy with them.
You will probably improve a lot, if not a complete cure. That’s the best thing you can try i would say.
Of course I looked at that thing
My two cents: high-normal testosterone level on its own doesn’t always translate to feeling-good. It’s that delicate balance in ratios (T:E2, E2:DHT, Cortisol:DHEA, etc.,). That’s why raising testosterone through lowering E2, for instance, tanks libido and induce myriad of issues including depression/anxiety. If this isn’t complicated enough, then consider that SHBG and Albumin and other binding globulins are equally important. That being said, normal is subjective. So, normal level for one may be abnormal for another.
A smart thing to do would be to get a bloodwork when you feel you best and not only your worst.
I was diagnosed as hypogonad nearly a decade ago, with a T level of only 25. I started TRT (Androgel), and my T level raised to the 600s and sexual capability returned to normal. Life was good.
Over 2 years ago I used Proscar for 3 months and developed PFS. I was Still on TRT and my T level was still in normal range, but sexual function was destroyed. Read my story for all the other PFS side effects I have been living through.
My personal testimony therefore is a man can be hypogonad , use TRT, and still suffer from PFS. They are not mutually exclusive, and TRT does not reduce or stop PFS from destroying a life.
I would not look for TRT to cure your PFS either.
3 Likes
Exactly. The term “PFS” wouldn’t even exist if all the problem was simply that Finasteride causes low T.
No. Here is my take.
Testosterone levels have been declining year on year for decades now. I saw the following quote the other day:
“An average 22 year-old male today has roughly the same testosterone levels as a 67 year old had in the year 2000. Average testosterone has fallen close to 50% in the last 2 decades, and nobody is talking about it.”
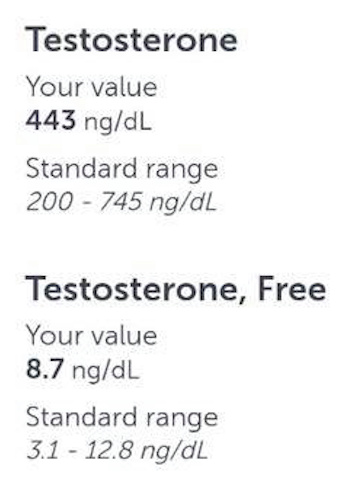
Want proof? Just take a look at the lab work below. The reference ranges are simply a calculation of the mean and standard deviation from a sample set of data. It is a representation that the average male is sedentary, fat, sick, SSRI’d, loaded with endocrine disrupting chemicals. It does not represent human physiology. It does not take into account receptor sensitivity to androgens. Just because your doctor says you are “normal” and “in-range” does not mean that your hormonal status is optimal for your biology.
Almost all of the symptoms PFS correlate with low testosterone. Logically, the treatment is therefore Testosterone.
Take the minimum effective dose to alleviate symptoms and maintain healthy blood work. If that means your Total testosterone sits at over 2000 ng/dl, then that’s where you need to be. Our bodies do not process androgens like a normal person. Our receptors are fucked up. The reference range is not applicable to us.
There are many stories of people recovering from PFS via Testosterone Replacement Therapy. Why waste your life because someone said PFS is incurable, who knows it could work out for you.
A correspondent I am in contact with who has PFS and avoids these forums like the plague sits at over 2000 ng/dl. He treated the symptoms, started testosterone replacement and within 6 months was cured.
In saying that, I do not think that Testosterone is the be all and end all for PFS. One must also consider the impact of neurosteroids, gut microbiome, adrenals, thyroid. It really does take a comprehensive functional medicine approach.
It’s worth a shot. Just my 2 cents. I am not cured yet by any means, but I wanted to share this information in-case it helps someone in any way.
Get well soon everyone and stay positive.
1. Free Testosterone Max: 350 pg/ml.

**2. Total Testosterone Max: 1836 ng/dl **
3. Total Testosterone Max: 745 ng/dl, Free Testosterone Max: 12.8 ng/dl. Literally a 50% drop in both Total & Free.
2 Likes
Thanx for sharing Alex. So, are you on TRT. If not, why not?
1 Like
I only started around 2-3 months ago. Still early days and taking it slow to titrate my dose up and dial in. Our bodies are sensitive. So I am taking my time and being careful. As I said, I am not claiming TRT to be a cure. I still think other aspects of PFS need to be considered like the microbiome, neurosteroids, epigenetics, etc. However the intent of my post was to shed light on the bullshit reference ranges and their drastic decline over time. Our bodies don’t respond to testosterone like a normal person as well, our recepors are fucked up. Anyway, If I do see improvements I will be sure to update and make a thread. My experience has only been positive so far, but nothing drastic. People say it’s hopeless, everythings been tried before, nothing works. Well in my eyes with that attitude you will remain sick for the rest of your life. Better to try and exhaust every option. I’m not trying to be insensitive in saying that, I know some people are very sensitive and can worsen their condition with treatments like TRT, and I am very sorry for your situation and truly am praying for your healing. But for a lot of people TRT has drastically improved their PFS, in my eyes it’s worth a try.
1 Like
Exactly. Thats what im trying to tell people and put my time and effort to warn other PFS cases even though i don’t have the same issues.
Read Moonman1’s MENT thread @Alex50 I think you may want to add Trest, if TRT feels underwhelming, you just have to push more, moonman still has the benefits of thas small usage of Trest with no sides. Aaron there is gonna try this too, but i think more people have to do this (Just for the sake of regarding the forum rules, please consider its risks yourself. Read the forum disclaimer first.) in order to see whats going and i think very likely, recover fully. Trest binds to AR’s very very strongly, it is not a coincidance that 1 people here completely reversed his PFS and one person got lasting benefits. I do support people should try diets first. To heal epigenetics. But most of us that is not enough.
This doesn’t even concern or interest me anymore, because androgens don’t work for me, i think i just want to help some people back, im very grateful of many people here who helped me along the years, but at the same time, many people halted others and me from recovery. I really don’t want to log in into this forum anymore until that day comes, it is just very sad, seeing people, not doing anything and wasting their lives because they are afraid now to use drugs again after their lives being destroyed by a ‘‘drug’’. I wish people encouraged me to experiment more because otherwise i wouldn’t waste 7 years of my life thinking time can heal me. Logically, there is no other way to fix yourself. You either try something which worked for others or stay with this disease. You are either a 0 or a 1. You can either say no or yes to something. Life is that binary in its core. Simple, plain, raw logic. Now im finally awaken.
It is the most ironic loop that a man can ever be pulled in. And the answer to PFS is to breaking yourself from the chains of this loop of fear, and grow some ‘‘balls’’. How ironic isn’t it, maybe a perfect life lesson with some twisted sarcasm in it?
4 Likes
Sometimes i saw Awor telling about his very low dose trt “protocol”, but i didin’t see people trying it. He knows a lot about this condition and have a lot of respect in this forum.
I probably wont experiment… i cant. Tribullus made me worse two times. The last time didnt sleep for a lot of days. I kept awake with no sleeping. I think there are two probably reasons: the betasitosterol on tribulus or the increase in AR expression due to tribulus.
Sorry for my english guys.
This was my “2 cents”.
1 Like
I hope I get something from TRT. One test came back very low, albeit an afternoon reading, waiting on a morning one. Just would need symptomatic relief.
btw this hypogandism v pfs stuff is nonsense. I can see that there are times when sufferers have gained enough sensitivity in their receptors or whatever over time that they could benefit from it. It’s also nonsense to say that nobody on the forum has got better from TRT.
1 Like
Than explain to me why there’s so many of us here that don’t respond to androgen therapy? I used TRT for 8 months and I was wasting away while on it! It’s not a cure for this condition depending on the severity. Good luck but if it doesn’t work don’t be surprised. If TRT worked than this forum wouldn’t exist.
What were your levels?
This is my $0.05.
We’ve some indication that enzymes that convert T to other steroids are severely downregulated.
T is virtually useless and it’s the metabolites of T that you need for most of it’s effects.
This is why for people without PFS someone with low T doesn’t need to have the symptoms of hypogonadism, if he have enough of the metabolites.
This study about another 5ARI mitotane is pretty good at explaining it.
Hypogonadism in mitotane-treated men initially manifests with a decreased free androgen index due to significantly increased SHBG levels that cannot be compensated for by up-regulated testosterone production as documented by increased total testosterone and LH levels. With time, gonadal testosterone production exhausts itself and circulating testosterone levels drop, accompanied by clinical manifestations of low testosterone including erectile dysfunction. However, testosterone replacement is often clinically ineffective and is complicated by an increased rate of gynecomastia.
The lack of conversion of testosterone to 5α-dihydrotestosterone also represents a logical explanation for the frequent clinical observation of relative inefficiency of testosterone replacement with regard to erectile dysfunction.
They also touch on the subject of how when mitotane users quit, after 2 years their 5AR activity is only back to 50% of what it used to be.
As I said at least in CSF this seem to be the same in PFS. The studies that’s been done has shown low DHT/DHP with an abundant of T. In that scenario, more T is unlikely to help. But there might be other manifestations of PFS and in their case it might work. PFS isn’t black or white.
2 Likes
What if you got PFS and then 15 years later out of the blue you develop hypogonadism, like me.