
What is cyclosporine and how does it work?
I would just simply suggest you search the forum/ Google
Immunosuppressant. That’s interesting.
I’ve been having high estrogen symptoms recently like: bloated gut feeling like there’s rocks in there, fat gain in hips, bad mood… Estrogen lab test claims it’s 5x over top range LOL. I’m not sure if this is a lab fluke or if it’s really that high ( I was taking some compounds which could cause a false high positive) but the symptoms are certainly there.
So to combat this I’ve recently started taking luteolin. It very very quickly takes care of all of them. One of the most powerful natural aromatase inhibitors. I’ve taken letrozole before and to be honest this works better without being overly harsh. It seems to more effectively inhibit the estrogen in various tissues, whereas with letro I got the feeling it primarily nuked your bones and joints and barely in places where you wanted.
I have better body composition with luteolin than letro and I feel far far better. Like it dumps all the water weight and gives me the same body composition and definition in my face that I had when I was 18. Small miracle. I’ve found it’s also an immunosuppressant now so I’m hoping it may give some 5-AR improvements if I take it for a length of time.
2 Likes
Why is your estrogen high? You on anything?
My testosterone came in at 1200, up from 690 in July. I think after my bicalutamide experiment all of my sex hormones shot up, but due to my 5 alpha reductase not being fully online yet, I am overconverting the T into estrogen. Kinda how people who go on TRT injections get estrogen issues sometimes.
I agree with you completely. I have written a very detailed theory about why and how this probably works and I have tried to explain people’s past negative experiences with DHT and T supplementation.
My posts in this thread:
DHT, especially targeted topical application, is the only thing that has worked so far for me. I have written about this in detail as well.
I have also asked people to try to challenge my theory and I have addressed all criticisms - successfully, I believe.
2 Likes
Just a small update…
I started this topic because I thought after a blood test my 5a-reductase was broken. But it later turned out that blood test was just an outlier. The info belows shows clomid/anastrazole/creatine raised my testosterone by 78% and my dht by 70%.
So long term use of finasteride (in my case 12 years) does not seem to inevitably cause 5a-reductase to stop working. (Also dr Goldstein said he thought my 5a-reductase was fine, despite that he earlier said finasteride destroys 5a-reductase.) Of course, other people could be less fortunate.
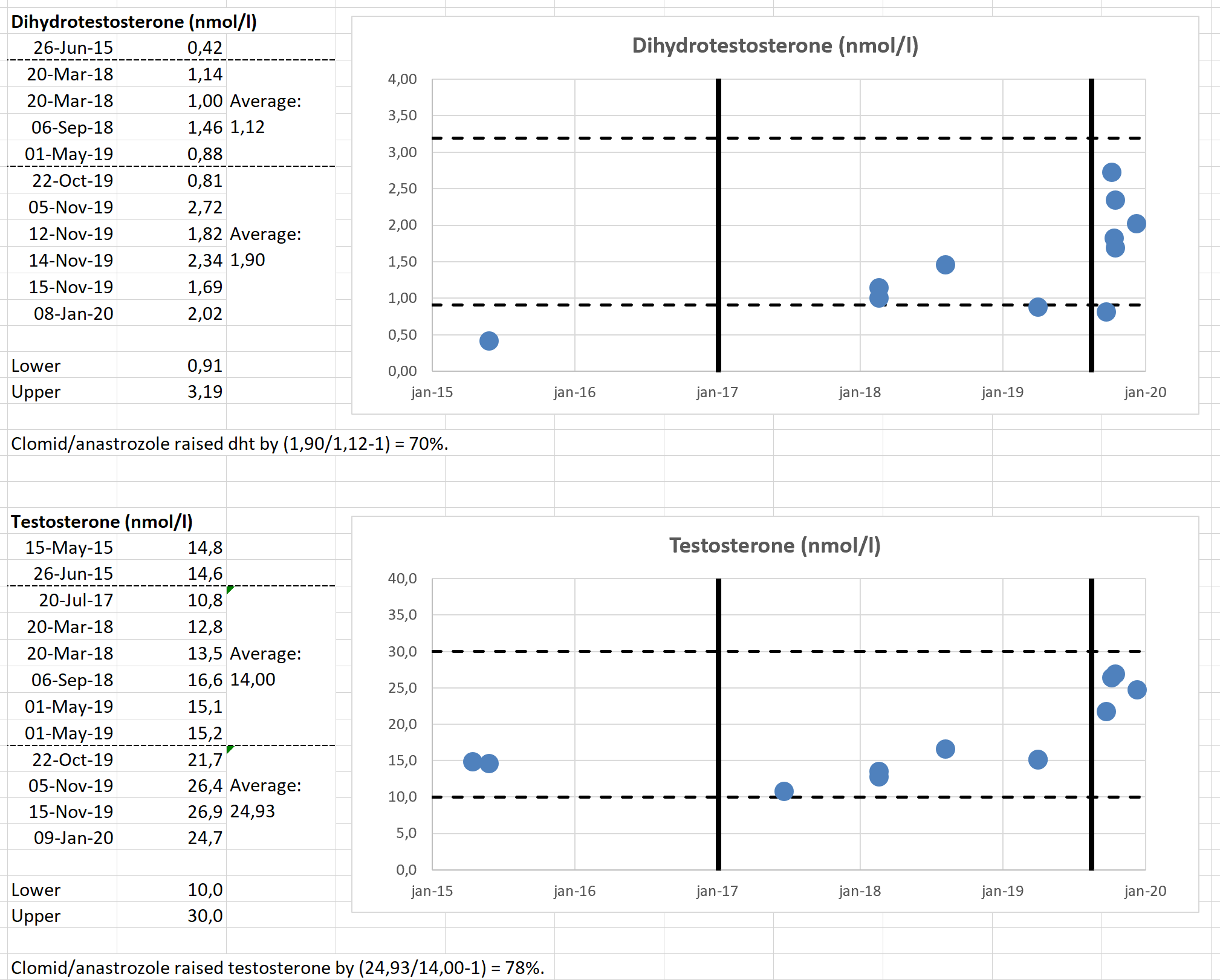
(First vertical bars indicate end of finasteride, second vertical bars indicate start of clomid/anastrazole/creatine.)
1 Like
Wow those levels are like those in bodybuilders who are taking anabolic steroids–their T and E levels go way too high! Be careful.
You may have only 5ar2 broken as I think is likely in PFS. If you artificially raise T, the other isoenzymes will still produce DHT and serum concentration will rise but the tissues where 5ar2 concentrated is may still be deficient.
In general, serum concentrations of DHT are not a good predictor of tissue concentrations - with or without boosting T. Tissue concentrations of DHT in key tissues where DHT is produced such as prostate are usually ten times as high as serum concentrations.
3 Likes
How are you feeling on the clomid / arimidex combo? How’s your estradiol?
Pardon the ignorance guys, but how do you get DHT levels tested? I’m under the care of a urologist as I was told the DHT levels can’t be measured?
How has this been working for you? Any improvement in symptoms? Any side effects? (Have you started losing more hair?)
Of course they can be measured. Google “labtestsonline” and you will see the hundreds of tests that can be done by Quest, Bioreference, Labcorp, etc.
1 Like
Crossroads, thanks. What would be a normal level of DHT to get an idea?
Remember that many people with PFS have normal DHT.
As to the range of DHT in the human body, google it because I am not sure off the top of my head.
I literary wrote about this three posts above as I have written about this many times elsewhere but apparently I am not getting this simple point across.
Serum DHT in normal ranges does not mean that DHT concentrations in key tissues responsible for sexual function are in normal ranges.
There is little correlation between serum and tissue concentrations of DHT (reference provided elsewhere), especially because tissue concentrations of DHT in key organs such as the prostate are (or need to be) ten times higher than in serum.
Further, serum DHT can be supplied by other tissues that are not deficient in 5a-reductase, such as the tissues that express 5ar-type 1.
5 Likes
Thanks! I didn’t know that but I’ll keep it in mind.
Actually, I hardly feel any change. Neither positive nor negative. If I have to mention something, maybe slightly gaining weight (1kg) and slightly thinning of hair.
I do have improvement in erectile function but that is most likely caused by a series of shockwave and prp treatments, see here and here.
Here is my estradiol:
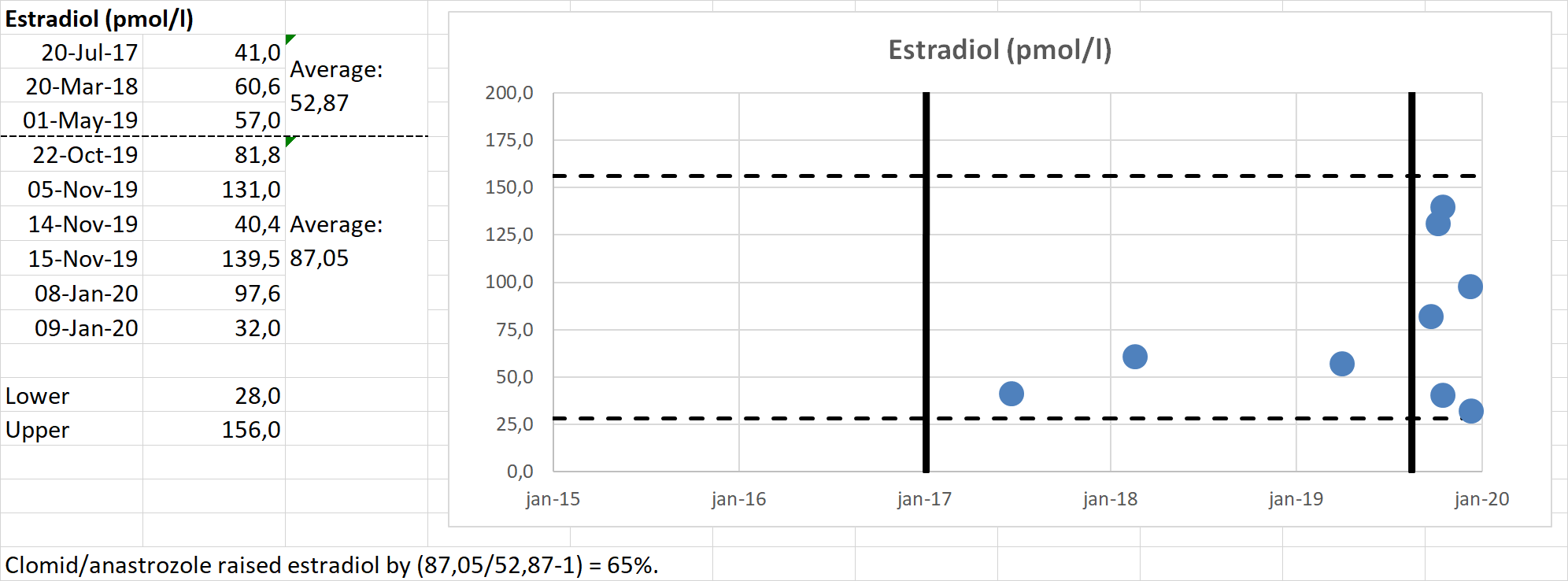
So despite anastrazole it is rising but still within limits and quite volatile. I am considering if maybe I should increase my anastrazole from 2.3mg to 3.5mg per week. (Dr says that is ok as long as estradiol does not drop below the lower limit.)
What’s your dose of clomid? Might be better off just lowering the dose
3,5x per week 50mg.
This summer I will lower it (probably to 3,5x25mg). But right now I would like to keep my dht relatively high because I recently had prp’s and shockwaves and maybe these are more effective if the penis has more dht. (Even though Sibelio warns the correlation between serum and tissue dht is low, I guess there is still some correlation.)
Its just a guess but I dont think these few months are harmfull; also dr advised 3x50mg.