You should give this a read, one of the few peer-reviewed publications which shows a successful treatment of PFS: https://www.longdom.org/open-access/postfinasteride-syndrome-about-2-cases-and-review-of-the-literature-2472-1212-1000170.pdf
The most relevant part: “the indicated treatment
consisted of HCGu 6000 UI/week, divided into 3 applications of 2000
UI/week, combined with Anastrozole 2 mg/week, divided into 2
intakes of 1 mg/week. Нis was done in order to hyper stimulate the
Leydig cells, elevate the levels of Testosterone and blocking the
aromatase, thus diverting the metabolism of Testosterone through the
5AR way (assuming it still had any remaining activity), without
compromising his spermatogenesis (Figure 3).
Figure 3: Indicated treatment. HCG: Human Corionic
Gonadotrophin. DHT: Dihydrotestosterone.
$іer 2 weeks of treatment he noticed some improvements, such as
less penile rigidity in a flaccid state, a more “warm” penis, increased
morning erections (without any changes in the rigidity of the
erections), some growth in penile girth, absence of post ejaculatory
asthenia, greater libido, increase in muscular tone and strength, and an
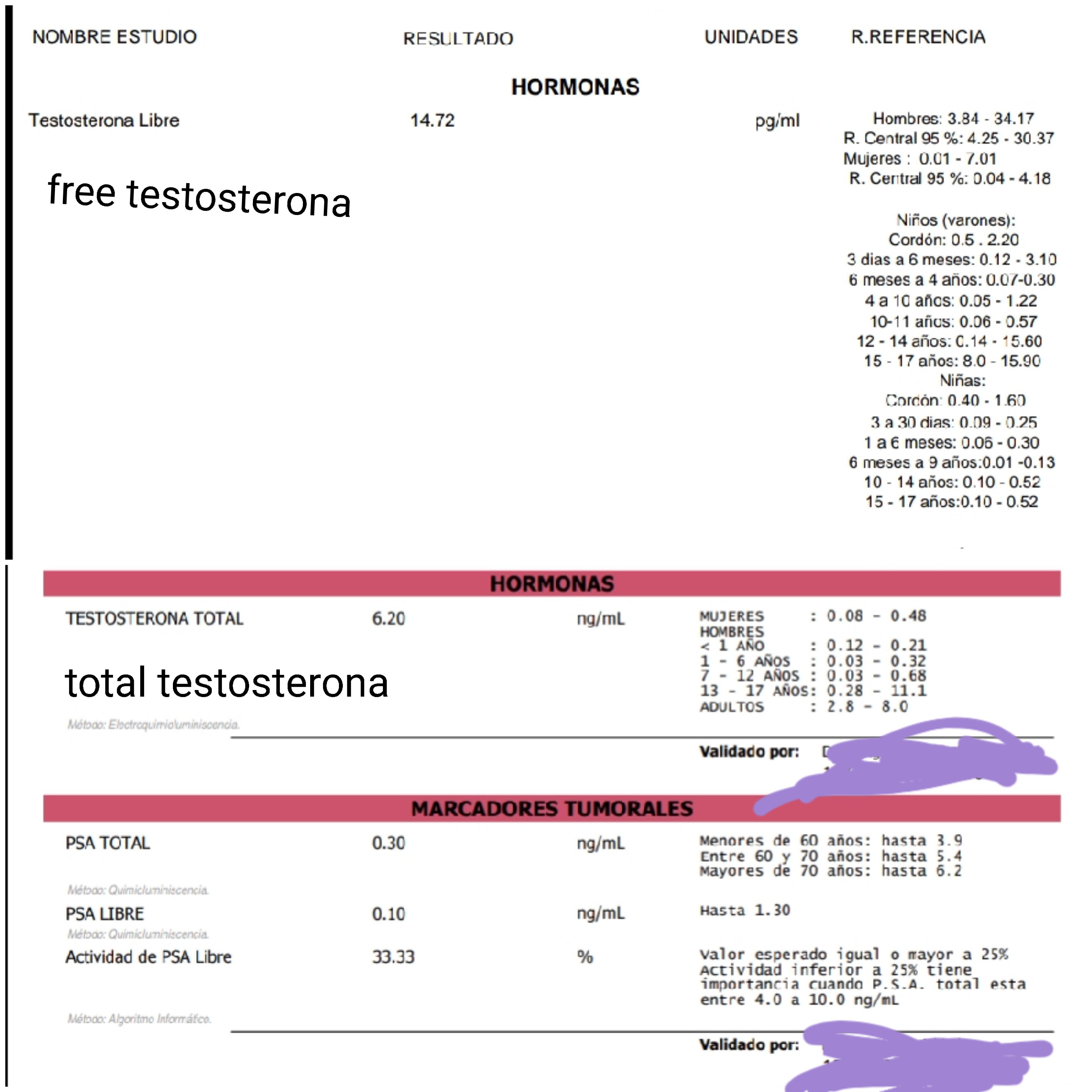
improved mood and self-esteem. One month later, a hormonal profile
was performed without DHT, showing a Testosterone of 10.2 ng/ml
(2.5-8.5 ng/ml), a bioavailable Testosterone of 6.14 ng/ml, and an
Estradiol in range, so we decided to lower the dose of HCGu to 5000
UI/week. Two months aіer this treatment modification, a new
hormonal profile was taken, which showed a Testosterone of 7.93
ng/ml, a bioavailable Testosterone of 2.42 ng/ml and an Estradiol in
range. Нis resulted in a more comfortable treatment (given that
HCGu is marketed in 5000 UI flasks as well as a higher sense of wellbeing. He is currently still under treatment, with a slow but steady
improvement in his symptoms, accompanied by periodic evaluation by
the Andrology team of the Urology department and the Psichiatry
department of the Hospital Italiano from Buenos Aires.”