My name is Alex Miller and I am studying biology -> specialization track: neurology and neurological sciences. I have been referred to this website by a good friend of mine who was using Propecia (Finasteride 1 mg) for 9 years. He never had any sexual side effects or other problems during this time. But about two month ago, he started having problems with cognitive function, forgetfulness, slurring of speech and depression. He went to several doctors and in the end a neurologist told him, that these effects come from the propecia. He then stopped using it and told me that if I have some time left, I should look into the matter. He started researching too and found this forum, where he said people named this side effect “brain fog”. Unfortunately, I just don’t have the time to read through this forum.
Before starting the research, I already knew that 5-alpha-reductase (5AR) has important functions in the central nervous system (CNS). So inhibiting it (by finasteride) might induce some side effects there. I will not address the possible sexual side effects but only the neurological ones. I will explain to you all what I have come up with so far. And guys: this is not looking good at all.
First of all, 5AR exists in two different isozymes: 5AR type 1 (5AR1) and 5AR type 2 (5AR2). 5AR1 is present mainly in the brain, muscle, liver and in sebaceous glands. 5AR2 is referred to as the “peripheral 5AR” since it is present mainly in the prostate, seminal vesicles, liver and hair follicles. Finasteride is a specific type 2 inhibitor and doesn’t inhibit 5AR1 in significant amounts. But here comes something that not many people know: 5AR type 2 is also expressed in very significant amounts in spinal chord motor neurons, actually in similar amounts found in the prostate (Poletti et al. 2003) and could have (damn it!: WILL have) an effect there. What kind of effect this is, will be explained soon.
Something else, that many people don’t know: Both isozymes of 5AR have more functions than just Testosterone (T) -> Dihydrotestosterone (DHT) conversion. They do the following conversions:
Testosterone -> Dihydrotestosterone
Progesterone -> Dihydroprogesterone
Deoxycorticosterone -> Dihydrodeoxycorticosterone
The latter two conversions are also inhibited by finasteride and so the production of neuroactive steroids is inhibited, since their metabolic pathway continues like this:
Dihydroprogesterone -> Tetrahydroprogesterone or also called Allopregnanolone.
Dihydrodeoxycorticosterone -> tetrahydrodeoxycorticosterone
These converions are catalyzed by an enzyme called 3-alpha hydroxysteroid dehydrogenase (3-alpha HSD). You can read about these neuroactive steroids on wikipedia in order to get a rough idea about them:
Altough it states there, that Tetrahydrodeoxycorticosterone is synthesized by 5AR1 in the brain, this is only partially true since, as explained above 5AR2 is also present in the CNS namely in the motor neurons of the spinal chord.
Now we come to the REAL concern: The inhibition of Allpregnanolone production. Altough Allopregnanolone can be produced in the brain by 5AR1, the CNS is also dependent on peripheral 5AR2. I quote from “Implications of neuroimaging for the treatment of epilepsy”:
Now to repeat again: Finasteride definitely inhibits allopregnanolone production in spinal chord motor neurons where mainly 5AR2 is present and also reduces allopregnanolone levels in the brain and other parts of the CNS since these parts are dependent on peripheral 5AR2 conversion of progesterone to dihydroprogesterone which is then converted to allopregnanolone by 3-alpha HSD.
The question is what the result of long-term allopregnanolone depletion is. Before you have to understand what the myelin-sheath of neurons is. The axon of neurones (both, peripheral neurons and neurons in the CNS) are surrounded by an electrically insulating layer: the myelin sheath. This is vital for fast and efficient impulse propagation on the neurons. I don’t want to go into details here. Fact is: Allopregnanolone has vital function in the myelination of neurons as seen in the following studies:
When you read these, you’ll see that the metabolic pathway of progesterone (inhibited by finasteride…) is vital for myelination and other functions in the CNS. In fact there are dozens of studies about the effects of progesterone metabolism and allopregnanolone on myelination.
Oh damn it! Didn’t we say just before, that the motor neurons of the spinal chord expresses mainly 5AR type 2 (inhibited by finasteride)? So there will be a negative effect of myelination there for sure!
Alright. Let’s see what the effects of demyelination are: Read Myelin ( en.wikipedia.org/wiki/Myelin ) . The most worrying effect is again demyelination of the motor neurons of the spinal chord which will be the effect of long term finasteride use:
Do you see those symptoms? Speech is affected, balance and cognitive awareness. This is exactly what you call brain fog here. The question is wheter this effect is reversable if you take finasteride for years. I certainly hope so for my friend although, you know, neurodegeneration can really be irreversible.
It has to be said, that these effects are of LONG-TERM use but probably WILL eventually happen after years of finasteride use.
Now, I don’t want to scare any one of you. I just want to give my input as a student of neurological sciences. Is it worth for you hair? My friend definitely regrets taking it.
Please ask if you have any questions but I don’t know if I have the time to answer them.
Someone should refer this guy to this forum… I feel like his input would be more beneficial here.
As for his specific statements, I feel like others will have more to say, in large part because I haven’t really experienced these side effects that much. I mean, I had some mental problems (still do occasionally), but I think that they largely stemmed from the same post-fin hormonal issues that have caused my far more problematic sexual sides. That said, I would point out that brain fog and the related mental problems are the one set of symptom where most guys on here seem to have seen improvent in the long term.
Made a post in the original thread about requesting his insights on this site.
For more insight into the allopregnanolone connection with cognitive symptoms and Alzheimers, as well as ways to hopefully reverse the damage, read the following threads:
Omega 3s (fish oil), antioxidants (grape, blueberries, pomgranate juice), cardiovascular excercise and mediterranean diet (lots of olives) appear to be beneficial.
Omega 3s in particular, as the brain’s neurons and white matter are mostly composed of fats… and omega3s can help with neuronal growth and repair… and cardiovascular excercise to promote bloodflow and neuronal health.
I’m hoping to work closely with Alex on this. He posted another comment to the thread today in regards to how demyelination may be tied in. Please read the thread:
"Alright guys. I had a quick look at the propeciahelp.com website. This site is a hell of a forum and I’ll need to read through the whole forum before making comments there. For this, I need a lot of time, which I, unfortunately, do not have right now. But I plan to do it soon when time allows.
But: I will write a brief comment on the condition of the guys experiencing permanent sides from finasteride:
I think, not only the mental side effects but also the sexual side effects are a result of the neurological damage from finasteride. Namely, demyelination of the motor neurons in the spinal chord. These neurons need to work otherwise you do experience sexual dysfunction. Your sexual dysfunction condition (I read comments like “there is no connection between the brain and the penis”) seems to be similar to the sexual dysfunction of multiple sclerosis.
Read multiple sclerosis on wikipedia. I quote the most important points:
Your demyelination just happend because of a lack of allopregnanolone which is synthesized by 5AR2 (yes, type 2 and only type 2!!) in the spinal chord and not because of an immune response. But the condition is the same.
Multiple sclerosis is a kind of Spinal Cord Injury. (see link)
I quote from there:
So here you go: Sexual dysfunction. I don’t think that an hormonal imbalance after finasteride use is the reason for the sexual dysfunction but rather the demyelination of the spinal chord which prevents impulses from the brain to reach the genitals. This fits perfectly to the description of “no connection to brain and penis” which isn’t like “normal” sexual dysfunction. If you have sexual dysfunction but nomal Testosterone levels after using finasteride, your damage is neurological for sure.
@Balance: Finasteride is a very potent inhibitor of 5AR2. Its inhibition is strong enough to stop hair loss (by a significant DHT reduction). So it certainly inhibits progesterone metabolism significantly too.
@Smitty109: I meant in the first post, that during all these years my friend didn’t experience sexual sides. But in the end he experienced them. They started at the same time as the mental ones. I didn’t write it clearly, sorry. It seems that both are an effect of motor neuron damage in the spinal chord.
To conclude: Finasteride has been tested by Merck before it got approved. It might be true that only 2% had side effects during that 5 year hair loss study. But neurodegeneration can happen over many years. And I bet they didn’t check for demyelination. I think that most people taking finasteride over the years will experience neurological damage (demyelination) in the spinal chord. It’s just that for some it happens in a shorter timeframe and for others it develops during several years. This is why Merk said, that no long term studies have been done, so that they don’t need to take responsibility for this kind of damage. But they certainly know that it will happen.
Someone please copy this post to propeciahelp.com. I can’t write everything on two different forums."
Anyways. I’m glad we have another scientist looking into the post-fin syndrome - that can only be a good thing. That said, I’m not sure how much I agree with his theory regarding sexual sides. As ScaredMale said in the Theories section:
And then even people like me, who haven’t had any really notable physical changes to our penis/testicles, often experience the sexual sides without some/any of the hardcore neurological symptoms this theory implies.
That said, given the sometimes varying symptoms described by post-fin sufferers, I’ve wondered for a while whether what we’re dealing with are actually a few separate fin-induced conditions. For example, maybe the bulk of people on this forum are dealing with various degrees of androgen insensitivity, while Alex Miller’s friend really is facing a largely neurological problem. Just a thought.
He isn’t a scientist to my knowledge, he’s a student studying biology with a specialization in neurology and neurological sciences (as he mentioned in his first post).
Here are some followup posts/replies he made in the original hairlosshelp.com thread:
Posted by Alex Miller:
"@Farrel:
The explanation to this is really easy: Real Multiple Sclerosis affects the brain and spinal chord. Most symptoms come from neurodegeneration in the brain then ED follows when the neurones of the spinal chord get demyelinated. Obviously, you see the effect of the brain damage first.
But: The brain has 5AR1 but the spinal chord has mainly 5AR2. Finasteride only inhibits 5AR2. I said the CONDITION at the spinal chord is the same. It’s not a real case of MS though since the brain is not as strongly affected of 5AR2 inhibition as the spinal chord. But I personally still think the brain is somewhat affected from peripheral neurosteroid inhibition although not as much as the spinal chord neurons.
This also explains why these neurological effects appear years after finasteride usage. It takes a longer period of time of allopregnanolone depletion for neurodegeneration to occur.
The symptoms of “brain fog” are definitely the same as demyelination of spinal chord motor neurons, as written in my first post.
Hope this answers your question."
Posted by Alex Miller:
"lol, do you think the spinal chord is just like an electrical cable? It is a highly complex structure. Within the spinal chord, you have specific regions, each has its function. 5AR2 is expressed in ANDROGEN SPECIFIC parts of the spinal chord.
I understand this is a rat study. But from the study of polletti at al. 2003b I know that the human spinal chord has similar androgen dependent structures.
And again: The brain fog symtoms are the same as the ones of spinal chord motor neuron degeneration. Is that so hard to understand? It even makes sense as cognitive function / speech behaviour are regulated by androgens too, so there will be an effect when the androgen dependent part of the spinal chord undergoes neurosteroid inhibition. Obviously, the strongest effect will be on sexual function as without impulse propagation through the androgen dependent structures of the spinal chord it won’t function properly. It’s not like you inhibit neurosteroid production and then you can’t walk anymore lol. I still think this theory is correct and people suffering these effects had demyelination going on in their (androgen dependent structures of the) spinal chord.
Of course while taking finasteride, sexual dysfunction can occur but THEN its because of an hormonal imbalance (low androgen levels / high estrogen levels).
Even when sexual dysfunction is not because of an hormonal imbalance but from demyelination, it CAN in fact be a selective symptom. See my last post.
People don’t seem to understand that Multiple Sclerose is demyelination IN THE WHOLE BODY while finasteride inhibits 5AR2 IN A PART OF THE SPINAL CHORD (in the androgen dependent structure). Surely, the symptoms of myelination there are selective. Again: The spinal chord is not a cable! "
Posted by Alex Miller:
Regarding the pseudohermaphrodites:
Smitty109 is right. It’s because they were born with this condition.
Why?
Puberty is the key. Pseudohermaphrodites never had DHT in their bodies. During puberty, certain androgen dependent structures in the body are activated by DHT. It’s the case with hair loss and also with other androgen dependent structures of the body such as parts of the spinal chord. A body of a pseudohermaphrodite works totally different since it never had its androgen dependent structures activated by dht. (And no: Testosterone can’t do this task.)
Normal men after puberty have totally different androgen dependent structures in their body. So finasteride’s effect is different too.
Posted by Alex Miller:
"Some people really want to take propecia for their hair. Ok. They can do it. I just wanted to enrich your knowledge about what actually happens in your body when you take it. I just don’t understand how you can use such a risky drug.
Posted by Alex Miller:
"Alright. Regarding the pseudohermaphrodites: I tried to explain it before but I will try to make it clearer now:
First, look at a normal male. Before puberty everything looks different. The body isn’t fully developed, the hormonal profile is different, the CNS is different too. During puberty, all of these things change and a lot of these changes are activated by androgens, especially by DHT. As the body produces androgens, genitals develop, sexual function is starting to work, the CNS develops which is also necessary for sexual function and for thinking and behaving like a male. The CNS looks different before and after puberty.
Now lets look at a pseudohermaphrodite. He goes through puberty too. But he is 5AR2 deficient so can’t produce DHT. He has less body hair, a different hormolal profile, and a different CNS since the androgen dependent part of the CNS which is activated by DHT hasn’t fully developed.
In the end, both went through puberty. But the normal male has another CNS, especially another spinal chord since it contains a lot of 5AR2 which the pseudohermaphrodite never had. So a pseudohermaphrodite doesn’t only look different, his CNS works different since it is not fully developed like the one of a real male. Point is: He is not only sexually different but also neurologically different.
Now: A normal male goes on finasteride and artificially changes his hormonal profile to match that of a pseudohermaphrodite. THEN, demyelination of specific parts of the spinal chord who have been developed with the help of DHT produced by 5AR2 will occur because the body is now, after puberty dependent on that specific part. It can’t function properly without it. A pseudohermaphrodite doesn’t experience such a kind of demyelination because his spinal chord is a different, not a fully developed one. The part that experiences demyelination in a normal male after puberty taking finasteride isn’t even present. His body can function without it because the spinal chord never underwent that change because he is 5AR2 deficient. It does function differently though.
You see: you can only compare the two (a pseudohermaphrodite and a normal male) if the normal male starts using finasteride BEFORE PUBERTY. But then both of them are actually pseudohermaphrodites.
Hope this is clear now.
Another thing I wanted to tell you: I researched on the internet (I know, not very scientific, but it’s still anecdotical evidence) in the hope to find other cases of multiple sclerose like symptoms induced by finasteride. And I came across these:
And there is probably a lot more. I found these two cases within two minutes. And they have been posted before I said anything about my theory. The latter case is about a finasteride user who took the drug for 10 years. He had the same “side” effects as my friend who goes through hell right now because of this drug. There definitely is anecdotical evidence which suggests that neurodegeneration takes place in the long term.
Another point: Some people still don’t understand that demyelination can be selective. I just tell you: finasteride is a selective 5AR2 inhibitor, so the depletion of allopregnanolone and therefore the demyelination will be selective too, namely in androgen dependent structures of the CNS.
Last point: I don’t know why people scream at me when I post wikipedia articles. I just posted them about demyelination, multiple sclerosis, spinal chord injury and about some neurosteroids. I posted them so you can have a look at them and roughly understand what I am talking about. It’s not like an experimental study on wikipedia which might be forged. These articles are about certain conditions and facts which I can assure you are true.
I hope some guys feel different today, when they put this drug into their body.
Posted by Alex Miller:
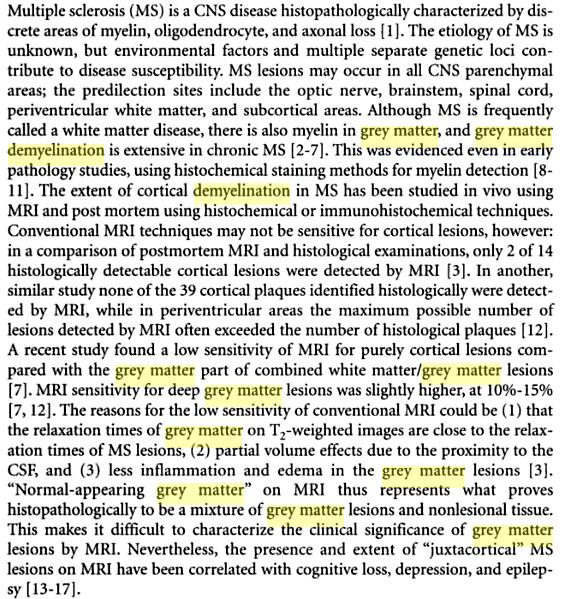
Guys: I continued my research and I think I finally see the big picture and I think I know what is going on and why several symptoms of finasteride side effects are similar to a “partial” multiple sclerosis.
As you can see, grey matter is present in the dorsal horn (=posterior horn) and in the ventral horn (=anterior horn) of the grey matter in the spinal cord.
So it seems, that demyelination in grey matter regions in the spinal cord occurs. This is the exact same demyelination process of multiple sclerosis. The only difference is, that finasteride induces selective demyelination in these regions whereas in multiple sclerosis demyelination takes place everywhere, including in the brain (people actually taking dutasteride undergo exactly this process…).
As you can see, in multiple sclerosis the gray matter is affected and so is it from selective 5AR2 inhibition in these spinal cord grey matter regions. As I said: The underlying CONDITION is the same.
Now, even more interesting is to know, that this is exactly the part of the spinal cord which is responsible for proper sexual function. See ninds.nih.gov/disorders/sci/detail_sci.htm about sexual dysfunction resulting from spinal cord injuries (MS = spinal cord injury and so is finasteride usage).
Quote:
Many of the finasteride side effects symtoms who most people think come from low DHT levels are actually from the finasteride induced spinal cord injury, including things like erectile dysfunction, ejaculatory disorders, and compromised sperm fertility. Aren’t these EXACTLY the finasteride induced side effects? People, wake up!
Another short insight about grey matter being responsible for multiple sclerosis from the Multiple Sclerosis Resource Center:
Furthermore, have a look at the attached screenshot. … Interesting point: Cognitive loss (“brain fog”), depression is mentioned too, what many people experience during fin intake.
I hope people understand this “theory” now. For me it is already reality.
I agree with what this guy says because I’ve maintained from the beginning that it’s neurological damage. I can feel this spot in my head that is numb, burned out and non-responsive. When I am having a good day, and this numbness is minimized, my sexual function and size of my unit is much, much better. To me it always felt like the signal was not getting all the way to my penis, thus my sub-par erections. When I can actually “feel” more, my penis becomes more engorged and the erections are of a way better quality. When I say feel, I mean feel it in my head. All sexual function starts in the brain first, then goes down the line to the appropriate areas. There may be some secondary problems from the androgen deprivation in the genital area, but when I’m feeling “on” it seems to be more neurologically rooted then anything.
"One last word about why such effects might be permanent: It’s because you don’t give your body a chance to recover for a long time. Sometimes people just start feeling the neurological damage by (in this case: spinal cord injury) after too much damage has been done.
Some studies demonstrate that neuroactive steroid production (neurosteroids like allopregnanolone, which is vital for myelination) is increased when the spinal cord is injured. This is the body’s reaction to the damage (in this case demyelination in the grey matter in the spinal cord). Usually this works perfectly in a healthy man in order to prevent such an advanced irreparable demyelination.
But you have to realize that while using finasteride, you not only do yourself neurological damage by inhibition of neuroactive steroids but you don’t let your body recover by a natural response of increased neurosteroid production by 5AR2 because you are inhibiting what is meant to heal you!
Surely, this can lead to permanent damage if you take finasteride without a break for many years.
Here is something similar but about the brain: liebertonline.com/doi/abs/10 … 005.22.106 . The same thing is true for spinal cord injury as shown in the above studies.
@smitty109: Many people already asked me to work with them regarding this issue. It’s just that right now I don’t have the time for this. I already posted a lot of relevant information about the neurological damage that finasteride does and affected people can study it/show it to their doctors or better neurologists.
When I’ll have some time left, I might publish a scientific paper regarding this issue. I think the world needs this. But right now, I just can’t (believe me, I wish I could) commit myself to this, because I am in the middle of some other important research, sorry."
Looks like these three hormones (?) play the main roll in our side effects. Is there a way to test them in your body? propeciahelp.com/forum/viewtopic.php?t=761 – this explains testing 3-androstanediol, right?
Testing allopregnanole isn’t that easy, right?
Haven’t heard about the 3rd. Maybe that can help us measure the type II 5AR activity?
And even if there’s a way to test it, there still isn’t a way to recover it… How can you make that hairloss enzyme to work on full power again?? I have feeling that it’s impossible and we’re hopelessly stuck in this shit.
I just fucking hope this guy spreads everywhere and proves people what finasteride is about, because he seems smart and argumented. Can’t just stand young people’s enthusiasm on curing their baldness anymore.
hey guys this has been a hot debate over at our forums
seems as though alex may have found a pathway that links finasteride use to multiple sclerosis as well (not to mention a great deal of other problems).
Meaning we, the people having weak 5AR, don’t have a chance restoring from faints and other unconscious states (alcohol poisoning), because allopregnanole is needed for that. We are very vulnerable and should be especially careful in life.
How do I explain my endocrinologist all this, when I want my 5AR activity to be measured?!
QUESTION: What kind of a break would you suggest, to minimize this risk?
"This is a really tough question. I have to admit, I can’t give you a proper response since this needs A LOT of scientific research as well as experimental studies. Up till now, not many people know that the nervous system is affected at all by finasteride use not to mention what exactly is affected and to what degree. Additionally, every person is different regarding this. Some guys are more prone to demyelination than others.
What I can tell you is this: In the second study of my just above post you can see that neurosteroid production increased 75 hours after transection. Of course, the gradually ongoing demyelination while using finasteride is not comparable to a transection. My guess is that as soon as neurodegeneration happens, which you can notice if you get “brain fog”-like symptoms, it is very, very, very dangerous to inhibit the healing enzyme 5AR2. When continuing using this drug under this circumstances, you scream for permanent effects. Of course, best thing to do is to not even let it go so far that you experience brain fog (this means some damage is going on already). Unfortunately for you guys, this can only be realized by stopping finasteride intake.
Another disadvantage of “cycling” finasteride is that it is not very healthy to change your hormonal balace on a regular basis. It’s just not healthy.
Something else (just avoid misconceptions): I am talking about finasteride here which is like candy compared to the dual 5AR inhibitor dutasteride. Dutasteride is literally poison, please guys, believe me. Anyone using this for hair loss is insane (personal opinion)."
Hm yes, this is all pretty fascinating. My question is that if individuals such as myself have only used finasteride for a week in their lives, and have dealt with the proposed demyelination effects for years thereafter, what is the missing component which has prevented recovery? In other words, if it is clear that the absence of 5AR2 has caused neurosteroid deprivation, what - if anything - is responsible for preventing those neurosteroids from still being produced post-finasteride, and regenerating the damaged nerve tissue/myelin.
Maybe we do have neurological damage which is not easy to heal if at all, however if this is the case, I am leaning more towards finasteride altering regular bodily production of 5AR2 or some kind of receptor blunting, keeping these and other side effects present in us.
It all jumps off the screen and fits, from demyelination symptoms to where in the CNS the damage would be rendered and thus cause. But does neurological damage explain changes in body composition to reflect poor-androgen function (gyno etc)? I don’t believe it does…therefore I am not convinced this is the complete story… just the beginning and middle.
Wonderful data nonetheless…and, additionally, not exactly something we did not know, but definitely something we did not do the math on. I think it’s of the highest priority to determine 5AR2 function in our bodies in these areas.
If the theory about androgen insensitivity via altered Androgen Receptor (AR) gene expression, desensitization or downregulation ever proves to be true ( propeciahelp.com/forum/viewtopic.php?t=2216 ), then perhaps AR function in those tissues where 5AR2 was inhibited by Finasteride never recovered, and thus androgenic function is not performing optimally/normally in those areas… thus extending problems experienced while on the drug even after quitting – sexually, physically, and of course, neurologically.
Correct, this is not the whole story, only part of it… but this thread does help further focus the specific impacts Finasteride can have on cognitive function, and the potential dangers to neurological health.
That said, Finasteride’s mechanisms of action target MANY bodily functions, organs, tissues and metabolic pathways. We are dealing with a multi-faceted problem here which requires investigation on numerous fronts – endocrinological, neurological, metabolism, hepatology etc.
As noted in the FAQ, stickies in various subforums and the FINASTERIDE STUDIES SECTION, the drug affects not only various hormones such as DHT, Testosterone, Estradiol etc… but also affects nitric oxide synthase, neurosteroid production in the brain and spinal cord, hepatic (liver) function/metabolism, and a host of other areas where 5AR2, AR and DHT are present.
No wonder many docs don’t know where to look and say everything is “fine” if Testosterone comes back mildly in range – they aren’t looking at the big picture, and don’t have the knowledge or awareness about what Finasteride really does. That’s why it’s important to print out scientific materials and bring with you to hopefully open their eyes, so they will take an interest in the matter.
That said, this is the Mental Side Effects section so we should try and keep this thread on topic – ie, allopregnanolone and myelination, brain and spinal cord etc.
for sure there are many areas where finasteride damaged our body but an interesting link is that some ppl had a full recovery by using natural progesterone or ghb that help neurologically and help to restore (progesterone) myeline in the nerves and to protect against the neurodegeneration in the brain as many studies proof.
so i wonder if from recovering the neurological areas will help to recover the sexual areas too by normalizing the hormone’s profile…cause don’ t foget that the body is a long chain of interactions (as we have seen).
Sent another question to the online doctors: a neurologist this time. The psychiatrist and GP-s haven’t been able to help. I asked the question exactly about this topic (allopregnanolone inhibiting) and even gave the link to the forum (hopefully she understands English). I’ll post, if she knows anything about this topic or not, when she answers. If I get something stunning, which I doubt after getting so many indefinite answers from the doctors, I will translate it.
Regarding white hair: Personally I don’t think that there is a significant correlation between whitening of hair and finasteride usage. One could argue though that since the mentioned neurosteroids (especially allopregnanolone) which are produced with the help of 5AR2, have anxiolytic (antianxiety) and anti-stress properties that stress levels are somewhat increased which could lead to whitening of hair. I admit that this is very far fetched though.
Regarding stretch marks: Stretch marks come from hormonal imbalances, especially from high estrogen levels. Women get them during pregnancy when estrogen is high. I suggest you do a blood test because if the stretch marks come from a finasteride-induced rise in estrogen this is worrying. You might have elevated estrogen levels which is not very healthy for a man and should be treated.
@beenthere: You asked me about sleep problems. Now: This is a very interesting point which fits very well with the proposed theory.
Spinal Cord Injury has actually been linked to sleep disorders. First I will quote from a study which proves this and then I will explain what exactly is happening.
Now, the explanation for this is again, the reduction of neuroactive steroid production because of finasteride intake. Allopregnanolone in the nervous system is very important for healthy sleep. The following study shows that allopregnanolone has many functions in regulating non-REM- and REM- sleep. The most important point here is that allopregnanolone prolonged REM Sleep latencies.
As mentioned above allopregnanolone prolonges REM Sleep latencies. When using finasteride, you shorten the REM Sleep latencies because allopregnanolone production is inhibited. Shotened REM latencies have been linked to depression which, guess what, is a common “side” effect of finasteride.
It has to be noted though that this study has been carried out with subjects who were already prone to depression. But it is still interesting and correlates well with finasteride induced sleep- and mood changes / depression.
@MikeYan1: How the hell can you make such a statement? Thank god I don’t have my friend’s condition. If you’d actually know what condition he is in, you wouldn’t have made that statement. I would never put a pharmaceutical into my body because of hair. Never.
@Bryan: You always come with the pseudohermaphrodites. Do you really need a study/scientific evidence about the facts that I posted above? Yes, I never analyzed them neurologically and I don’t think they have ever been. But what I said is common sense and logical. It’s not just “an explanation” I have come up with - it’s the explanation.
Again:
Pseudohermaphrodites don’t exprience demyelination in the spinal cord because their spinal cord isn’t fully developed because of 5AR2 deficiency. They don’t experience demyelination in other parts of their body because 5AR1 is responsible for neurosteroid production there.
Normal male with postpubertal finasteride intake experience selective demyelination in parts of the spinal cord, namely in the parts where 5AR2 is responsible for neurosteroid production. They don’t experience demyelination in other parts of their body because 5AR1 is responsible for neurosteroid production there.
The point is: 5AR2 has 2 tasks.
T -> DHT conversion
Neurosteroid production
Task one takes place dominantly in the prostate, seminal vesicles and other androgen specific parts of the body. Task two takes place dominantly in the nervous system, namely in androgen specific parts of the spinal cord which are also linked to sexual function.
Common sense says that post-pubertal finasteride intake by a normal male is a different than 5AR2 deficiency from birth. You have to realize that you are actually the one who has to prove to me that they are comparable.
Pseudohermaphrodites are not a good model for post-pubertal finasteride intake of a normal male. Period. End of story.
Another post by Alex:
Some proof that 5AR2, highly expressed in the spinal cord, is actually there particularly for neurosteroid production and not for T -> DHT conversion.
The proposed theory is getting more plausible by the second. Again, we see that there is an upregulation in neurosteroid production in the case of neuropathy in the spinal cord.
This proves what I already said yesterday: By using finasteride, you inhibit the enzyme that is supposed to heal you! If this is done for a long time, permanent damage to the nerves in the spinal cord could be the result.
Posted by Alex Miller:
Yes it isn’t essential for the pseudohermaphrodites because they are pseudohermaphrodites. They don’t have normal sexual function because of an only partial puberty. So they don’t need the part of their spinal cord which is there for sexual function. Like they have underdeveloped genitals, parts of their spinal cord is underdeveloped, and still like the one of a normal male child before puberty.
See, the genitals are developed by DHT during puberty. So are parts of the spinal cord. You know that their genitals are underdeveloped. For the same reason, parts of the spinal cord which need DHT during puberty for developement are underdeveloped and therefore don’t need 5AR2. A normal male before puberty doesn’t need 5AR2 “there” either because that part doesn’t exist. That’s why no demyelination occurs.
But you are right. I admit I can’t prove it but I think it is true and I think it sounds plausible and makes a lot of sense. You can’t disprove it either. I tried to find studies but nobody studied their spinal cord but only sexual characteristics.
As somebody mentioned before, a normal male who takes finasteride post-puberty and has side effects that the pseudohermaphrodites don’t experience, proves that they are in fact different. And this points exactly into the direction of what I said.