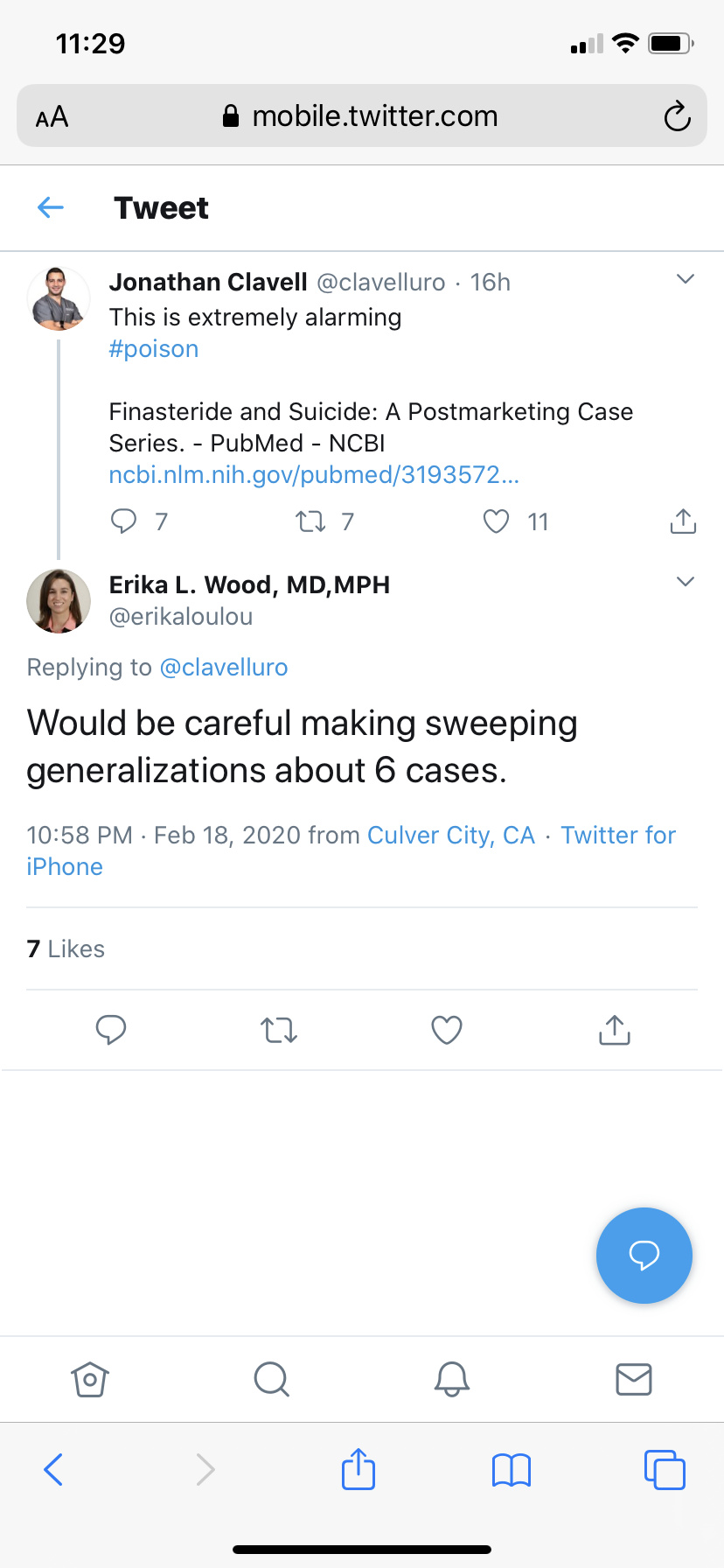
Looking at those replies. When patients express clearly their doctors do not properly clinically record their situation, how could the numbers game they are hoping to play ever be useful? We know from the patients themselves and their families that these cases are incompletely recorded, so we cant get statistical power that way. The disease is too rare, and our last suicide - amongst many others - was not clinically recorded.
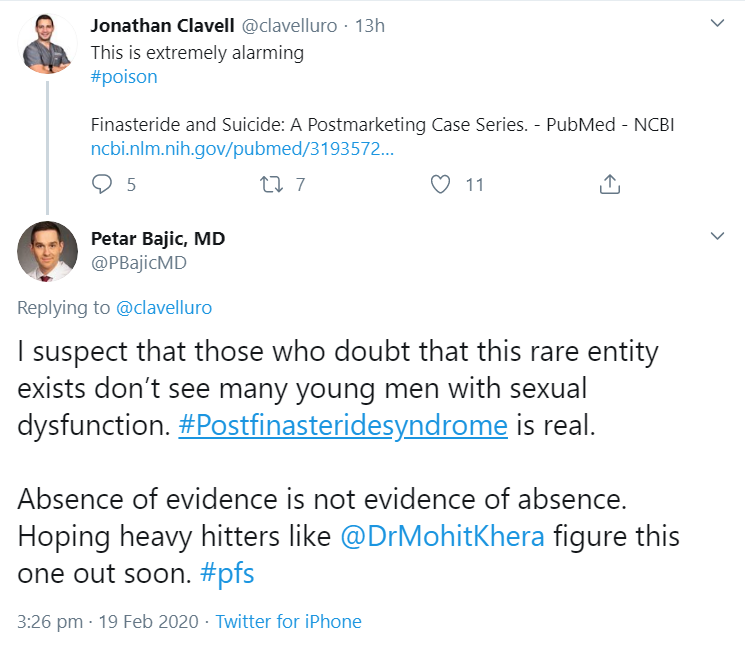
As Prof Irwig mentioned in his paper, a disease of this rarity reaching signal in a placebo controlled trial would require a trial of a scale and duration that could never be achieved. A rarity in predisposition in line with a well-recognised genetic andrologic disease - say above one in 350,000 - wouldn’t make three cases in a million consumers. We know PFS is more frequent than that, but it is still extremely rare.
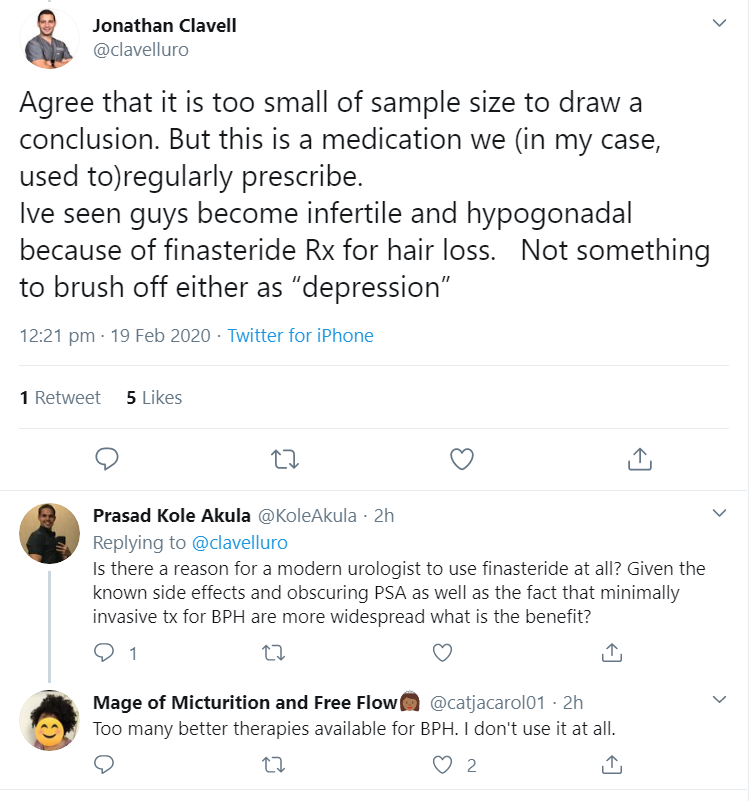
Therefore, when the clinical experience of our patients is to generally be entirely dismissed (180 surveyed reveals extreme dissatisfaction denoting a dangerous situation per Short Assessment of Patient Satisfaction), what on earth are we meant to do? Die quietly while a few urologists declare the numbers not very strong, carefully mentioning only the symptoms that aren’t undeniably physiological? It is absolutely risible in 2020. I truly wonder how they would feel if it were them, or their child, suffering this horrendous disease and they saw such indifference. Anyone outside of this sorry situation would hope such professionals to be there to protect and help young people who had their lives snatched away by clinical ignorance.
For those wondering why we bang on about numbers in the survey, here’s the reason. We need as strong data as we can get, especially given the inherent biases of purposive non-random sampling.
I should say however despite the disappointment of the usual handwaving, it’s very clear the situation is entirely different from how it was. There are some clinicians there with a clear awareness, concern, and even first hand experience. Very heartening.

 safe to say we’re in good hands
safe to say we’re in good hands