Please forgive me if i’m a little hard to follow, my head is a bit foggy at the moment.
OK so I guess to start i need to mention there are essentially three stages involved:
-
EARLY HIGH CORTISOL STAGE
-
WANING MID STAGE
-
ADRENAL EXHAUSTION
List item
-
So a normal person produces about 20 mg of cortisol a day, those with unbalanced lifestyle – (stress +++ and sleep deprivation) have their cortisol production rise ten-fold to 200 mg each day. Helps you maintain normal blood sugar levels, creates energy, is anti-inflammatory, modulates immunity, stabilises BP and controls mood.
-
In this mid-stage, cortisol is still high but starting to fall, and three other hormones decline:
SEROTONIN - problems with depressed mood, DHEA - associated with decline in immune function, decreasing sex drive and malaise and fatigue, MELATONIN - poor sleep.
-
chronic overstimulation of the adrenal glands finally leaves the adrenals depleted, and unable to perform their protective role.
Issues include:
Aberrant CNS function - anxiety and nervousness, and an inability to relax.
Gut problems - surging adrenaline disturbs the gut’s ability to produce various important digestive enzymes and decreases gut motility (often diagnosed as IBS)
Thyroid problems - precipitates thyroid imbalance as they work together
Hypoglycaemia - aberrant insulin levels
Sorry if im going on too long, but i think it important to know the regular course of events - it goes without saying that PFS confounds mainstream approaches as you know.
So, preferred treatment and testing as i understand it consists of the following:
A balanced diet, reduced caffeine, nicotine, sugar and alcohol intake. Getting plenty of sleep, exercise and relaxation.
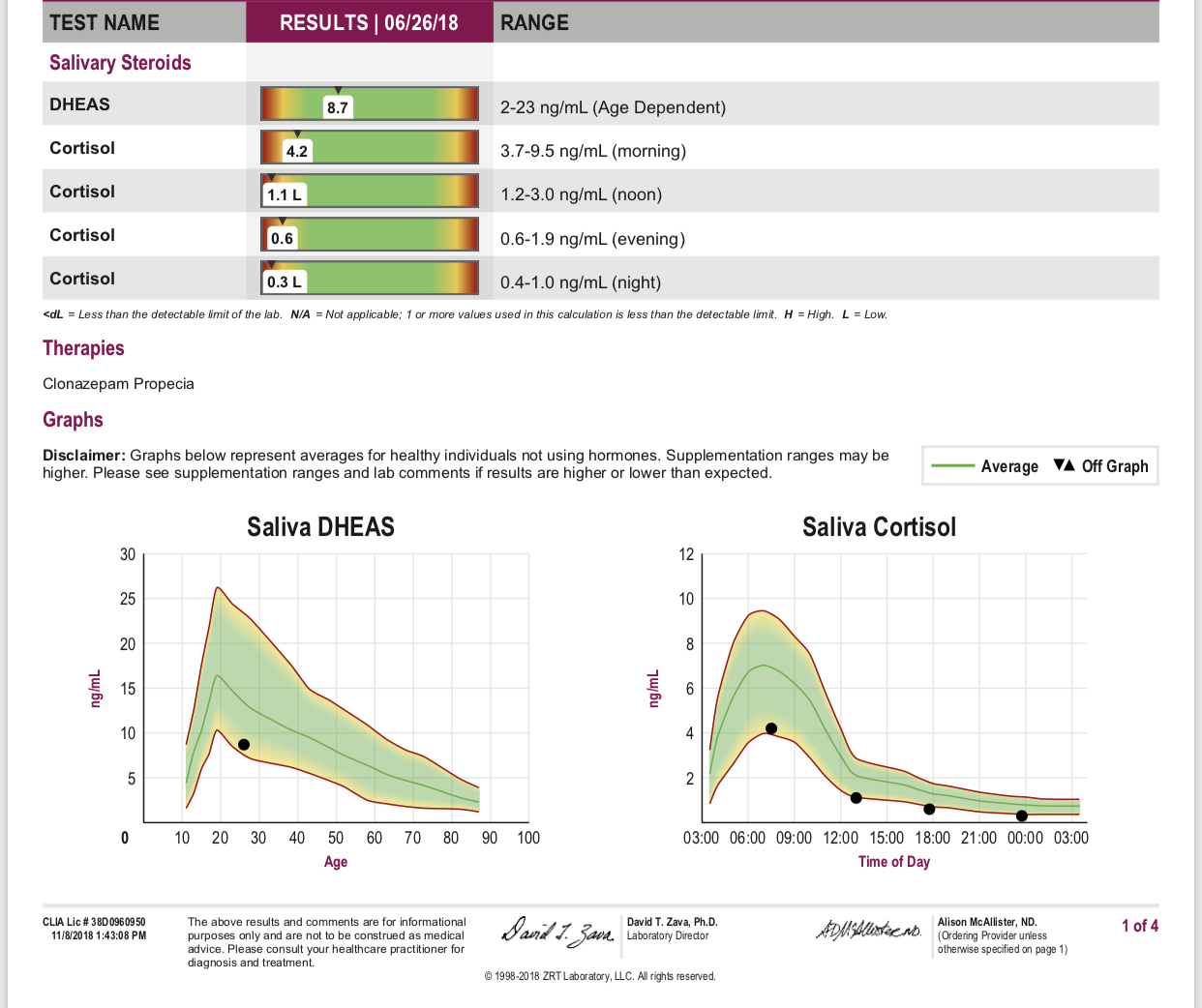
DHEA and Cortisol are the two main hormones of interest as these two hormones are continuously secreted in response to long term stress, and they regulate metabolism and thus energy production. Aldosterone is another adrenal hormone which is easily tested and worth considering. It regulates sodium and potassium levels so contributes towards regulating blood pressure.
Anyway in terms of levels - Cortisol (blood test) an ideal range is 300 -500 nmol/ L (NB:“ ideal” is higher than “average”) DHEA ideal range 4-12 µmol/L.
Treatment - nutritional supplementation:
Please be careful taking any of these - if your levels are normal it is not advised.
Adrenal Corticol Extracts - These are also called adrenal cell extracts. They are liquid or powder extracts of the adrenal cortex. It is important to understand that they are not replacement hormones, rather that provide the essential and natural constituents for adrenal repair – this includes nucleic acids (adrenal cell RNA and DNA) and concentrated nutrients in the form and proportion used by the adrenals to properly function and recover. Actual adrenal hormones as such are present but only tiny amounts.
There’s a product available in Australia from Thorne Research - www.thorn.com
Adrenal Cortex (Bovine) 50 mg one capsule, one tab three times a day - this dose can be increased (under medical supervision).
Several other complexes are available with supplements that support the adrenal gland, and often the thyroid as well. eg adrenoplex, adrenotone, S.F.M. XCel, adrenergy forte, adreno enhance. Their ingredients are variable and may contain the following nutrients, and adaptogen herbs withania and rhodiola as well as other herbs.
NUTRIENTS - examples in adrenal complexes
Tyrosine 300 mg
Iodine (as potassium iodide) 100 mcg
Selenium (as selenomethionine) 75 mcg
Vitamin E 50 IU 42 mg
Zinc (as amino chelate) 5 mg
Inositol 200 mg
Biotin 39 mcg
Pantothenic acid 1.5 mg
HERBAL SUPPLEMENTS – examples in adrenal complexes
Withania somnifera root 1.5g 1500 mg
Rhodiola rosea root 200 mg
Panax quinquefolius root 1.0 g
Stimulating herbs such as Gingko Biloba should be avoided, as the adrenal in particular need softer, supportive care particularly in the early stages of recovery.
That’s probably all i can say on the topic - It may not be of help, but i sincerely hope you can at least take something away from my ramblings.