
I ordered my neurotransmitter and urine hormone tests today. I’ll post my results might take a couple weeks
3 Likes
I’ll check it out, thanks. if i go ahead I’ll post my results.
2 Likes
That’s great that you ordered the ZRT urine hormone metabolite and neurotransmitter test. It will definitely be a couple of weeks before you get the kit, supply the sample, send it back to them and get your results. I’ll have to find moreplatesmoredates on you tube so I can see what it’s all about.
So I’m 36. I have been living with PFS for ten years. I took dutasteride with I was 22 for a month due to prostate enlargement. I did not get PFS on the dutasteride or while coming off the dutasteride. I speculate that the dutasteride may have done damage. But I felt perfectly fine up until age 26 when I took Saw P In a “testosterone booster” supplement from GNC. I got hit with all the “PFS type” sexual sides while on that Saw P containing supplement. I came off the supplement and the sexual sides did not improve.
At age 29 I took Saw P again but this time I took a straight Saw P supplement. I got absolutely crushed at exactly the two week mark of being on it. I knew something was wrong when my digestive system literally “turned off”. I came off the Saw P and the severe constipation remained and I developed severe insomnia. I put dutasteride as my poison when I made my account. I believe that even though my health and my body could handle the dutasteride when I was 22 to the extent that it did not give me PFS sides I still think that it did a lot of damage. Setting me up for failure with my first Saw P mishap when I was 26. Someone else already asked about this and I will update it to dutasteride and Saw P to avoid more confusion.
I’m familiar with how it’s speculated that PFS, PAS and PSSD may have similar mechanisms. I’m on another forum where a very knowledgeable person does a good job at trying to find differences in the three. I personally think that the three do have different mechanisms. I’m aware that Ronnie99 is post accutane.
A little while back I seen Ronnie99 post urine hormone metabolite test results that looked similar to ones that I had done. It caught my eye because I had just recently got my urine hormone metabolite test results back and because I’m not familiar with anyone else who got this test done.
I seen that his urine testosterone, epi testosterone, and 3a-diol were high like mine. So it is true that what I really wanted to know is if another saw P, Fin or Dut case would show similar patterns in their urine hormone metabolite test results as mine. And I never went to Ronnie99 specifically asking him to get the test. I just seen that he got the test on his own apart from my test. Naturally it still caught my eye that Ronnie99 who’s post accutane showed identical and similar results as it pertained to urine testosterone, Epi testosterone and 3a-diol. Accutane is a 5AR enzyme type (1) inhibitor exclusively or mainly. I hope my memory serves me correct on that because I did not have a chance to research that statement so I’m just going off of memory on that.
It’s a shame that you were prescribed all three poisons without getting proper warnings. Good luck with the appointment with your PCP and please keep us posted. I’m looking forward to your results on the urine hormone metabolites so that we can see if there is a solid pattern here with the metabolites among people who took 5 AR enzyme types (1) and/or type (2) inhibitors
Thank you for doing this (fingers crossed for pattern)
1 Like
I havent got money to just throw around, but I done this test about 2-3 years ago, so I think its best i do it again and also the pregnenalone sulfate test you recommended. Will post results when I have them.
This could be interesting as we got a few other guys giving it a go which with about results from 5 people you could definately see somewhat of a pattern if there is one which will be presented.
Speak soon.
1 Like
Wheres the pregnenalone sulfate test?
Yeah Im 26 now. I took finasteride a year ago noticed side effects immediately, didnt know what to expect thought it was just my body adjusting to the medication. Ended up taking it for like a week before I reported side effects to my doctor who said stop taking it. Of course it was an online doctor who cant help at all and takes no responsibility to do so. Just sends me to my PCP who just thinks its anxiety even though I have messages with my doctor reporting the side effects. It gave me cognitive issues, eyes, muscles, skin, fatigue, slight ed but that is the least of my worries. My balls ached for like 6 months even after stopping. It left me in a state where Im not able to work like I used to.
It has to be either an endocrine problem or neurosteroid problem. The solution seems so close but so far away.
Im surprised you were able to somewhat handle the dutasteride or anyone for that matter. I know Ashton Kutcher took that for over a decade
1 Like
So your issues are mainly cognitive ? you did not get smashed with the sexual sides? just slight? and you did not get the insomnia and digestive issues?
creatine HCL helped me with the lost muscle mass. Never got all the muscle back in my legs but almost all of it.
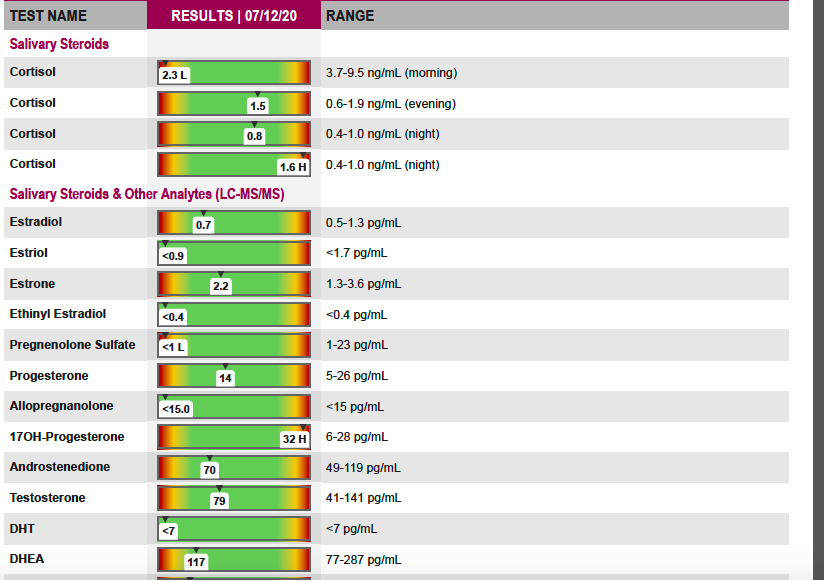
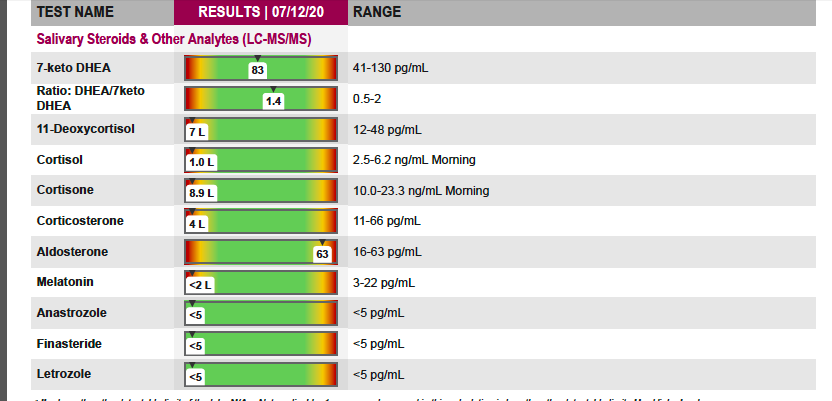
Here are my ZRT LCMS saliva test results. This is ZRT labs test that tests for Pregnenolone sulfate. You can see that I am flagged low in it. ZRT actually made this test for doctors to monitor their patients while on Finasteride. Note that the saliva allopregnenolone reading in ZRT’s salvia hormone test cannot tell you what exactly your allopregnenolone levels are. That’s why the reference range for ZRT’s salvia allopregnenolone is ambiguous. ZRT’s LCMS testing technology is not currently sensitive enough to provide an exact reading of allopregnenolone from a saliva sample. The only thing that the allopregnenolone reading is good for in this test is that it tells you if the amount of allopregnenolone in your body is high or now. So when looking at my saliva allopregnenolone reading in this test all it’s telling me is that I don’t have high allopregnenolone. So based on this we know I am not producing high amounts of allopregnenolone in spite of my body getting rid of a high amount of it in my urine from the other test
Yes main sides are cognitive issues, muscle tremors (leads to exercise intolerance), visual snow, after images, dry red eyes. I guess ball ache could be considered a sexual side. Slight ed.
So your body is not producing allopregnenolone. What role does it play as a neurosteroid? Is the 5aR enzyme related to it?
Also strange if your body isnt producing allopregnenolone then why would there be so much in urine?
Looking at the reference range of the allopregnanolone on ZRT labs LCMS salvia hormone test we can see that the reference range is as follows:
LESS then 15 pg/mL
So when I first seen this I was confused. So I emailed the owner of ZRT lab and he explained it to me. When a lab uses a reference of “Less then 15 pg/mL” they are saying that anything less then 15 pg/ml is normal and anything over 15 pg/mL is high. This type of a reference range is only telling you if your value is high.
In this case because my allopregnenolone was not high it’s considered normal as far as this reference range is concerned. However it’s not actually telling me what my allopregnenlone level is. It’s just telling me that it’s not high. The doctor/researcher/scientist who owns ZRT lab explained that in certain instances when patients go on Finasteride their allopregnenolone can go high which can make someone feel shitty so this test to an extent can be used to monitor patients while on Finasteride. But like I said this tests is not telling me if I am producing low amounts of allopregnenolone or not. It’s just telling me that I do not produce high amounts of allopregnenolone.
Ok so now based on this test I know that I don’t produce high amounts of allopregnenolone. But I am still left thinking “do I produce low amounts of allopregnenolone”?
So the reason why I actually got ZRT’s urine hormone metabolite test was to see if I was low in allopregnenolone or not. Again I knew that I was not producing high amounts of allopregnenolone from ZRT’s LCMS salvia test but I still did not know if I was producing low amounts of allopregnenolone. So I got the urine test knowing that ZRT’s urine hormone metabolite test (the one that you ordered) would not only tell me if I was producing low amounts of allopregnenolone but that it would also tell me exactly what my urine allopregnenolone levels are. Why? Because ZRT’s labs urine hormone metabolite test has a full reference range for the urine allopregnenolone value. It’s not just saying “less then such and such is normal” because it’s not high. It’s actually providing a normal reference range like we are use to seeing in our blood hormone labs.
So now I get my urine hormone metabolite allopregnenolone results back and see that I am peeing out top of the reference range level allopregnenolone levels….
Obviously common sense makes me ask my self this question:
If I know I am not producing high amounts of allopregnenolone per the saliva test THEN WHY AM I PEEING OUT HIGH AMOUNTS OF ALLOPREGNENOLONE???
I’m either producing normal or low amounts of allopregnenolone and I am peeing out most of it? Well why? If I was producing high amounts of allopregnenolone I would suspect to see high amounts of in my urine. Produce more in my mind means pee out more. But I am peeing out more in spite of not producing high amounts of it. This is what catches me eye. Get my logic?
To answer the rest of the questions:
Progesterone converts to 5a-DHP via the 5AR enzyme. Then 5a-DHP converts to allopregnenolone via the 3a-HSD enzyme.
Obviously I understand that a lot is unknown about allopregnenolone and the implications with messing with it. Which is why there should not be a drug that messes with it without the impact of messing with it having been properly studied. They do know that allopregnenolone is a positive allosteric modulator of the GABA receptors. My understanding of what this means is that not only is allopregnenolone agonizing the GABA receptors but it “modulates” them. In my mind this means that allopregnenolone is making sure there is enough action on the GABA receptors adjusting their sensitivity in a way that allows them to respond “positively” to GABA. Opposed to pregnenolone sulfate which is negatively modulating the GABA receptors hindering the GABA receptors response to GABA. It’s also my understanding that the GABA receptors need a proper balance of positive and negative modulation to work properly. The GABA receptors should not be too sensitive but they should not be too insensitive. Which is why I am assuming “mother nature” gave us neurosteriods that both positively and negatively modulate the GABA neurotransmitter receptors. So this is why I am theorizing that I have a GABA receptor imbalance. Because I do not appear to be producing enough pregnenolone sulfate while I am peeing out top of the reference range amounts of allopregnenolone. This to me suggests too little negative modulation of the GABA receptors which may be why my body is peeing out as much allopregnenolone as possible in order to avoid too much positive modulation in lack of negative modulation. If you read about what can happen when the GABA receptors are not balanced things go bad. Like seizures and all kinds of horrible things. So maybe my body is smart enough to stop as much positive modulation of the GABA receptors as possible by getting rid of it’s allopregnenolone in the urine knowing what the outcome will be if the allopregnenolone hits the GABA receptors with not enough negative modulation (pregnenolone sulfate)
Disclaimer:
This is all theory based on my own labs. So I am not claiming to know what PFS is. I am simply trying to explore my theory further in others
What are your neurological symptoms?
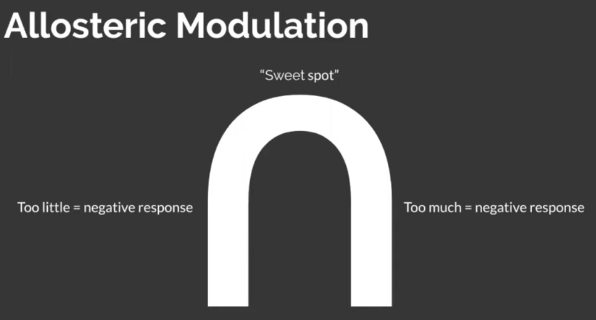
I agree an imbalance in allosteric modulation of the GABA-a receptors is likely in PFS. There is a sweet spot. What are your symptoms? My theory is;
- Too little allosteric modulation, low allopregnanlone, results in anxiety, feeling wired, overstimulation and insomnia (this is what I’m dealing with),
- Too much allosteric modulation, maybe high allopregnanlone, results in anhedonia and apathy. These are the individuals that do not respond to alcohol and benzodiazapines.
I fall into the first class of individuals, I find great benefit in using benzodiazapines, ashwagandha and progesterone, which are all postiive allosteric modulators.
It would be interesting to see if you fall into the latter class of individuals given your high allopregnanlone per your urine test. The people in the latter class may benefit more from negative allosteric modulators, like pregnanlone sulfate.
2 Likes
Here is ZRT labs sample saliva LCMS test:
Here is ZRT labs saliva LCMS test on their Website:
Scroll down a little and you will see it. It’s under saliva testing options and listed as:
“LCMS Saliva Steroid Profile – E2, E3, E1, EE, PregS, Pg, AlloP, 17OHPg, Adione, T, DHT, D, DS, 7keto, 11DC, C, Cn, Ccn, Ald, Mel, ANZ, FIN & LTZ”
Here is the company that told me that you guys could order it from. They said that you can text, call or email them and ask to get the test through them
978-475-7779
This is “ ZRT’s gem” and they make it the hardest for patients to get out of any of their other tests. You have to get this through doctors or specialty pharmacy’s. The company above is a speciality pharmacy who told me over the phone they will sell the LCMS saliva test to PFS patients without a doctors order. They told me over the phone that they will simply send you the test kit and that you would pay ZRT directly after sending ZRT lab your saliva sample. For the record I have spent hours upon hours on the phone with doctor offices and specialty pharmacy’s and this is the only one I could find that told me over the phone that they are willing to simply send you the LCMS saliva test kit with out a doctors appointment. For now though let’s just focus on your urine hormone metabolite test though so that we don’t get confused.
I’ll post the instructions shortly regarding how to supply the urine sample correctly . We want to follow the instructions to the T so that we can trust the results.
Well if we are right about what we have in mind then perhaps all of my symptoms are neurological. Thinking along these lines the first thing I tried was increasing serotonin. I seen that the amount of serotonin in my urine was not in the optimal range. So I took serotonin precursors 5-HTP, L-Tryptophan and serotonin co factor vitamin B6 in order to see if it would increase the amount of serotonin that I was peeing out.
We know that we don’t know exactly what are bodies are producing based on what the body is getting rid of in the urine. Because what’s in the urine is what the body is eliminating of a certain thing. Not the exact amount being produced.
But it is telling us if the body is getting rid of high amounts of certain thing. It’s also giving us a clue as to what we are producing.
For example we know that it’s not the cause that I’m producing extremely low amounts or no Allopregnanolone. Because how could I be producing extremely low amounts of or no Allopregnanolone if I have top of reference range levels of it in my urine. I cant eliminate something from my body in high amounts in my urine if I’m producing no or low amounts of it.
I think this is an important point because in Melchangi’s study the PFS group had extremely low amounts of Allopregnanolone in their CNS and in their plasma. Melchangi’s Allopregnanolone findings in his study make it appear that the PFS group in his study are producing low amounts of Allopregnanolone. This suggests that the 5AR enzyme and or the 3a-HSD enzyme are not working. BUT what if the PFS patients in his study had high amounts of Allopregnanolone in their urine? Would this change his way of thinking? Because now we would know the PFS patients in Melchangi’s study had low CNS Allopregnanolone even though their bodies are still producing it. In that case it would seem like we are getting rid of the Allopregnanolone (even though we shouldn’t be getting rid of it) in order to keep it low in the CNS.
So when I increased the amount of serotonin I was peeing out my gut turns back on and my constipation goes away. Three times now I have stopped the serotonin supplements listed above and my constipation comes back. And when I start taking those specific supplements again my constipation goes away. So I think in my case the constipation is neurological in the regard that my body can’t properly regulate serotonin for some reason. If you google serotonin you will see that most of the bodies serotonin is produced in the gut and that it stimulates intestinal movements.
I also got severe insomnia after the second time I took saw p. And severe insomnia again recently after taking several amino acids including the amino acids that I listed above for serotonin production. The recent insomnia was very similar to the insomnia that I got from the Saw P when I was 29 seven years ago. Except this time I did not take saw P or a 5AR inhibitor. I simply took amino acids that convert to neurotransmitters in the body. So in a way I gave my self PFS from taking amino acids recently. This is why I think that it’s neurotransmitters. The insomnia that I got recently from taking the amino acids had me up for 8 days straight followed by weeks of hardly any sleep . So this felt neurological
I get every PFS sexual side. These sides got worse from the amino acid combination I was taking as well. Amino acids increase neurotransmitters. So the sexual sides to me feel neurological.
But it’s confusing. Because the serotonin amino acids that I listed above cure my constipation while the combo of all the amino acids I was taking essential cause PFS in me . So for me it seems like a neurotransmitter imbalance.
Another thing to consider about pregnenolone sulfate is that not only is it negative allosteric modulator of the GABA receptors but it’s also a positive allosteric modulator of NMDA receptors. The GABA receptors are the bodies main inhibitory neurotransmitter receptors and the NMDA receptors are the bodies main excitatory neurotransmitter receptors. Imbalance in either GABA or NMDA receptors could cause these issues and the bodies main inhibitory and excitatory neurotransmitters should be balanced with each other. If you read about GABA and NMDA receptors you will see what I mean
So low pregnenolone sulfate (like I’m flagged low in) could implicate issues with both the GABA and the NMDA receptors. Because it’s a positive allosteric modulator of the NMDA receptors and a negative allosteric modulator of the GABA receptors. So maybe I have a NMDA/GABA receptor imbalance. I’m hoping someone else will be low in saliva pregnenolone sulfate in order to increase the likely hood that I’m onto something.
What are your symptoms ? Which of your symptoms does benzodiazepines, ashwagendha and progesterone help ?
Benzodiazepines are the only thing out of the arsenal of things that I tried to treat my recent PFS like insomnia with that worked. When the recent insomnia relapse was at its worst benzodiazepines are literally the only thing that would help it. I wonder though if the benzodiazepines will ultimately make imbalanced GABA receptors even worse though. If this theory is right we also need to think outside the box. Maybe if the GABA receptors lack negative allosteric modulation the GABA receptors stay down regulated/insensitive in order to avoid the reaction of having only positive allosteric modulation. Maybe the body in the case of lack of negative modulation pees out as much Allopregnanolone and 3a-diol as possible and makes the GABA receptors insensitive somehow. If this is true then in theory taking benzodiazepines which are prescription strength positive allosteric modulators of the GABA receptors only makes things worse in the long run. I don’t know though just throwing out ideas…
For me benzodiazepines only helped me sleep in my insomnia state. Of course now that Im getting good enough sleep I’m not taking the benzodiazepines. Benzodiazepines did not help me with the constipation or the sexual sides. So if taking prescription strength allosteric positive modulator of the GABA receptors does not help my constipation or my sexual sides I’m assuming that this means another factor/factors are at play that causes these issues. I have learned a lot though about my imbalances. Positive allosteric modulation of the GABA receptors temporarily helps the insomnia. Increasing serotonin production in the GUT helps my constipation. So I’m obviously looking for the key to the sexual sides and I suspect the answer also lies in neurotransmitters and neurotransmitter receptors
In a perfect world if gods on my side I increase pregnenolone sulfate and everything becomes balanced and falls back into place
1 Like
My symptoms include feeling wired, overstimulated, feel fried in the brain, inability to tolerate stimulation (like scrolling the internet or playing a stimulating video game makes me extremely wired), issues sleeping, etc. My GABA is heavily dysregulated. Benzodiazepines make me feel 100% normal, but I’m obviously not going to depend on this. I’m picking up some high quality CBD oil next week to try instead. Low dose fluoxetine did help initially, but I’ve decided to come off as I don’t want to be using an SSRI given my sexual dysfunction. It would be interesting to see if what a urine neurotransmitter test said, although I don’t believe they represent what’s in the brain or CNS at all. My current efforts are focused on hormone therapy and fixing my gut microbiome.
2 Likes
I feel you very much. That overstimulation from everything is exhausting. I become stupid and anxious. Like you’re drunk without positive effects.
Do you feel something like the inability to plan or thinking abstract, like something is physically blocking you from complex thoughts? And have you noticed any pattern in these symptoms fluctuations? According to my diary, they are fluctuating in a cycle of around 28 days. So I think it very much related to steroids.
I hope all is well and you received your urine neurotransmitter and hormone metabolite test kit with no issues.
The first thing I recommend is not rushing into providing the sample. Just open the kit, leave the paper cards that get exposed to the urine in the zip lock plastic bag that they come in and get organized. Let it sit for a couple of days, learn the instructions and what to avoid eating prior to taking the samples. If the instructions are not followed correctly the data we get is useless because we wont be able to trust the results.
Watching this instructional video on how to provide the urine sample is a must prior to providing the sample. You can click on this link and scroll down to urine collection video. It’s called 'urine collection video" and is the 3rd one down. Ignore the salvia and blood collection videos above it because for now they are not relevant. it’s easy to follow video.
A couple of things about the video:
The video is saying that the better of the two methods is to hold the sample cards and urinate on them. DO NOT USE THIS METHOD. The video is wrong. This is not the better of the two options.
Instead use the urinate in the cup method. Use a glass cup. Clean the cup with soap and warm water. Make sure you go over the top with making sure that you wash all the soap out of the inside of the cup after cleaning it. Use clean paper towels to dry the inside of the cup down. Then urinate in the cup all the way to the near top. Dip the paper card into the cup exactly how the video shows you to do it but dip it all the way to the last black line. Directly up to the last black line and take it out of the cup. The video will show you how the card flips open and how to let it dry. Follow the instructions in the video exactly how it’s saying to let the card dry. There is four cards which means 4 samples through out the course of the day. Each time clean out the glass cup with warm water and soap and dry with clean paper towel before urinating it again for the next sample. If you have any questions about how to handle the paper cards after they are saturated in the urine and how to let the cards dry before folding them closed please let me know. I can answer all questions in vivid detail so we don’t F this up.
I will also post the written instructions that explain what not to eat prior to providing the sample. You will also have a copy of these instructions that come with the kit. I figure this is enough to digest for now and like I said don’t rush to get it done. We are better off waiting a couple of more days before we have the results and getting it right. The rush is getting the kit in the mail to get it back to ZRT after it’s completed and packaged up. Not providing the sample. No rush for this. The pre paid shipping label is a 2-3 day delivery back to ZRT so they get it timely before the sample goes bad. And ZRT tests it as soon as they get it
Yes I was thinking just that. I received it on friday and was reading the instructions. Wanted to take my time with it. You sent good information for me just now and I will let you know when I send them out.
1 Like
This is me %100. I can use maybe a tenth of my brain power. Can’t keep up intelligent conversations, can never think of words, socially withdrawn, don’t feel connections with my peers, tired and drained mentally all the time. If I sit and do nothing I feel fine. Yay
If anyone has been treating this group of cognitive sides , step up and share.
1 Like
The more I experiment with amino acids the more I see how strongly they affect PFS for me for the good and bad
Aminos have made me worse in the past so I stay away from them
Dieting either gives me diarrhea or constipation so I stay on a fairly normal diet to keep things moving. I tiny bit of metamucil and a half a multi vitamin every other day seems to do the trick.
Also I avoid cows milk, rich portions of gluten, rich portions of tomatoe and soy.
Every hormone I have tried has had a negative effect- immediately converts to estrogen, haven’t tried an AI because of the anecdotal stories of people getting worse. However i know nothing about them. Antidepressants , wellbutrin made feel like shit , low dose fluoxetine immediately gave me ed and took away my attraction to women within a week and made me feel like a zombie. So what the studies about it not having the effects of ssri at the low dose is bull shit at least for me, made me poop incredibly well but that was it, so I mmenditarly stopped.
1 Like