Has anyone tried strong androgens at very high doses for a short period of time to wake up androgen receptors ?
And I don’t mean proviron, masteron or testosterone.
I mean trenbolone or mtren.
Did that work ?

Has anyone tried strong androgens at very high doses for a short period of time to wake up androgen receptors ?
And I don’t mean proviron, masteron or testosterone.
I mean trenbolone or mtren.
Did that work ?
I have tried tren, halo, NPP… etc. for me nothing good came from them.
I do think there is logic in shock therapy. Bipolar Androgen Therapy is used sometimes for another condition with likely the same mechanisms as PFS. It take 6 months with one massive injection of test cyp per month in a pre shut down state. The aim of this is for constant change and shock.
I think the steroid recovery’s have a commonality being they often include large fluctuations in hormone levels.
Keep in mind for many androgens can worsen PFS.
Good thing you already tried them, I was about to place an order for tren and mtren.
That’s really a shame that even the most steroids on Earth can’t solve such an issue.
I really don’t feel that well with e2 only, it just makes massages and any touch to the skin feel incredible, but something is definitely missing in my personnality on this protocole.
I wonder if MENT or Dbol would give the best of both worlds as they are strong androgens with a massive estrogen conversion.
Dbol felt less harsh for me likely as a result of high conversion. It’s not beneficial however.
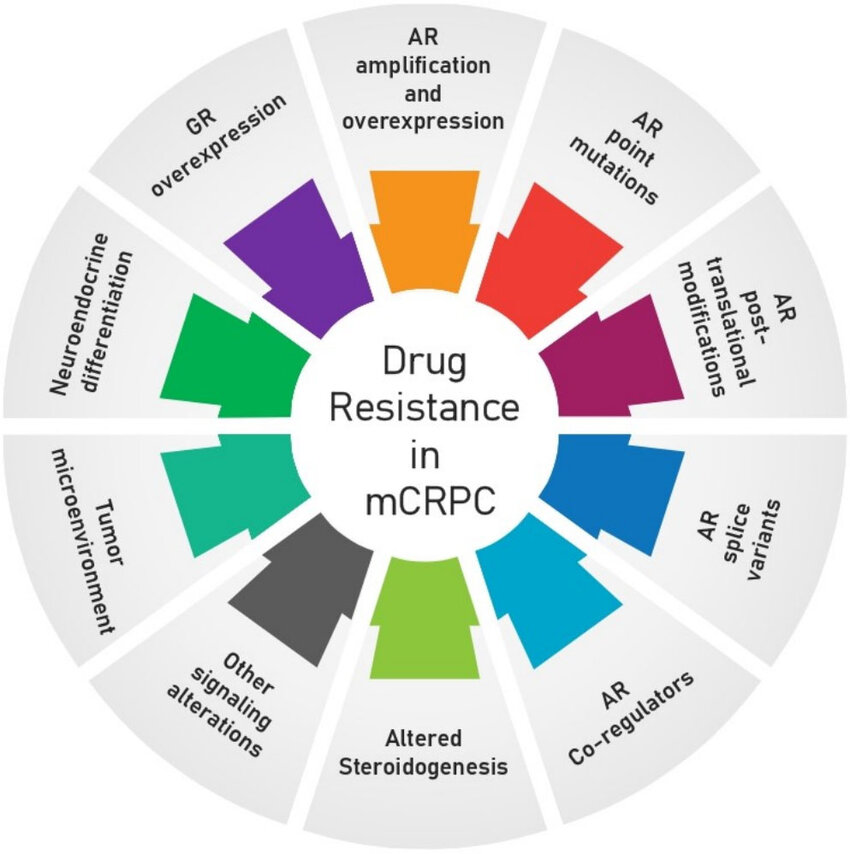
I recommend watching Dr Alfonso and Mitch video on YouTube. That explains it well. The benefits in what I do results largely from lowered androgens (in my case castrate levels). It is about matching the AR : androgens equilibrium and in PFS affected tissues AR is hypersensitive to androgens. I believe something crazy like 100 times more sensitive. In the literature castrate levels are optimal for growth. Also in the literature estrogens, anti-androgens and other hormones bind to AR in agonist way (not like in normal tissues without the issue which do not allow binding of other steroid ligands to its binding domain).
Why aren’t we all hyper-sexual you may ask from the above? Well hypersensitive tissues to androgens at the overexpression level results in suppression of tissue growth in a normal androgen level environment. Picture a bell curve - there are increased benefits until you hit the peak and then the direct opposite occurs beyond that point. We are way past the peak and there is likely some gene that is not regulating AR back to normal.
In a certain way it’s way easier for me because PFS is so severe and widespread, that the response to low androgens is therapeutic and brings some androgenic effects I would have previously got from androgens.
For further reading I recommend anything current in mCRPC. But at least watch the video with Dr Alfonso.
Below is a good start.
Because of AR over-expression. It is also reasonable to assume ER under-expression in the affected tissues. So not only AR:Androgen equilibrium is off but also ER:Estrogen.
So estrogens can help certain symptoms as well.
Basically my goal has been since about 3 years ago now to castrate myself and increase E2 levels to fit the new equilibriums. It works exactly as the literature explains and even though logically I was expecting a lot, I was still completely taken back by how extreme the improvements were.
In order to castrate simply taking large amounts of estrogens is the safest way. The treatment would be called Estrodiol HRT monotherapy and would take time to work as a form of castration.
There’s one guy with a similar background as you (post exemestane syndrome of sorts).
Idk if he speaks the truth but he tried mtren specifically. Mtren is the most potent androgen available afaik.
https://raypeatforum.com/community/threads/finally-cured-from-post-finasteride-syndrome.33215/post-990391
Your experience with e2 is very interesting to me.
Have you had blood tests done on your protocol (lh/fsh, test:e2, shbg, ceruloplasmin etc markers are especially interesting)?
Also, AR could be manipulated by manipulating GR (similarity of structure; zinc finger etc). The same applies to ER but via a different pathway (ER-CB1-GR and GR-PGE2-aromatase).
I think microbiome/or even just gut dysfunctions are in a big part androgen:estrogen mediated but also conversely dybiosis disrupts proper binding of androgens to AR and estradiol to ER. Check this: https://raypeatforum.com/community/threads/transdermal-testosterone-solvent.52479/post-980856
Yes, so regarding helping the gut. Many people in the forum refer to it like chicken and egg scenario.
Poor gut health definitely is a knock on effect rather than the root cause without a doubt, however that’s not to say a lot of symptoms can’t be related to the gut and therefore can’t be helped with that type of focus.
I’ve had benefits from a 10 day water only fast, also from artemisinin, and a bunch of supplements that can help the gut in theory such as berberine and curcumin. Not much long term improvements unfortunately, but the fast has the most benefits.
I do think there is great benefits to be had from FMT, but I wouldn’t spend loads of money expecting a lot.
Manipulating hormones had the most beneficial impact on my gut health, which for me has been about lowering hormones.
One knock on effect that comes with AR overexpression is reduced ability to detoxify properly. AR overexpression is even linked to higher heavy metals and so treating it with heavy metal chelators and anti-oxidants can help.
I got great benefits from cycling DMSA + ALA 24/7 around the clock for 3+ day cycles. During the cycle I’d feel weird changes in the brain like movement of things and then change in personality to a much better and more relaxed version of myself.
I also got really good benefits from twice weekly injections of glutathione mixed with Vit C. My skin started to glow and my mind was just working way better.
You can order these from china for not too much - it’s a commonly used produce over in Asia for skin whitening purposes.
Edit - I should also point out any benefits I got from anything other than estrodiol has been also during taking estrodiol. This matters because I respond as I should to things after E and I don’t crash from anything if I’m on E apart from androgens.
I’ll have a read from the link soon.
I have tried mifepristone high dose for a week before based on the in vitro evidence for mCRPC it shows because of the GR antagonism. Unfortunately it didn’t work alike the human trails, but I did feel some nice benefits for a while from that week.
I think mifepristone is worth a shot. I ordered it from ru pills and had legit stuff.
Re blood tests I had them done 6 months ago and I’m due another test in July from my endocrinologist. 6 months ago bloods showed <0 (undetectable) testosterone and estrodiol was within the female range. I never got the papers so can’t comment further.
Very interesting - so your hpa is basically fully inhibited yet you feel fine. Thanks for sharing.
The ER-CB1-GR I’m not too sure about. ER-CB1/CB2 relationship is well established. But it gets complicated by the fact that ER also has two forms ERalpha and beta. Also, I’m not sure if the connection is CB1-GR or CB2-GR (both probably).
I really dislike the endocannabinoid system haha. Very dangerous to play with because we don’t have enough available CBr antagonists. It’s part of the “emotional” experience but atm risky to manipulate.
Actually, considering endo CB ligands are also made from arachidonic acid, just like prostaglandins, we can connect that to PGE2. And here glutathione is the biggest player (cysteine metabolism crucial) so we basically come to the conclusion that glutathione redox restoration is what every protocol should strive for.
Mife is very interesting. Both due to PR and GR antagonism. But if someone wants to play with GR then mife should be taken with progesterone I think. Either way, I agree with you.
Mifepristone by itself. Short term antagonising the GR can reset the stress system and can be useful for anyone here with “psychotic depression” characterised by chronic elevated cortisol. GR also works in tandem with AR and has almost identical function. Our condition is likely also characterised by overexpressed GR.
I don’t see much hope for a cure outside of science which can be directly correlated to CRPC research, so I use that as a screen nowadays and have more or less stopped researching with the improvements.
The reason why I feel so good completely shut down is because of the etiology of PFS / hormone refractory cells. In some literature the optimal response change to androgens in vitro was from 0.1nm to 0.001nm. Quite staggering. We are in a way lucky to have such a strong tie with CRPC research but at the same time 5 or so decades and many millions of dollars has not cured that condition. There has been dozens of red herrings where various approaches work in vitro but not in humans. The main hope imo is from gene therapy and that’s a decade or so away.
In the time being I treat and live on.
Mifepristone helped the lawyer recover after years of fin and ofs
It definitely is a hopeful method. I know that one guy without a doubt was lucky with this one and fixed himself.
There were a bunch of people that also tried it using non-perfect sources. The negatives some pointed out seemed to me to be signs of re-activating highly expressed AR rather than fixing the AR expression issue because the signs were of hyper-androgen nature e.g rapid increase in MPB. It’s a shame it didn’t help with the tissues they wanted to fix. It worked for areas like their hair follicles lol.
Many years ago now I had one window of recovery and it wasn’t like before PFS it was also likely highly expressed AR tissue activating. I had rapid re-growth of genitals to way beyond the norm, the highest sensitivity and libido I’ve ever had. What caused this period for me was a sudden drop in hormones after stopping a steroid cycle. I don’t advocate trying because I tried many times after without luck. It obviously didn’t fix the root issue either, it just somehow re-activated highly expressed tissues for a period.
I understand your castrate strategy in order to re-match the overexpressed AR equilibrium. It is rational.
By the way, what do you think happened in the bodies of people who recovered over time? A few PFS patirnts recovered within a couple of years unless their recovery stories are untruth. It seems difficult to explain it by decreasing androgen level caused by aging.
I think in many cases from the crash onwards other independent mechanisms in the body can likely adapt somewhat.
So in my case from 0 hours sleep per night after a year I could have broken sleep waking up every 30-60 minutes and sleeping total of 3-4 hours on a good night. What improved? I think not the root issue but maybe my ability to create the necessary sleep hormones to a certain extent.
In most cases of improvement I would say the body likely has adapted in certain ways and also the psychology of chronic conditions like this has its own twist.
Firstly, people find a new normal and can start to forget the pre-PFS state to varying degrees.
Secondly, people want it so bad and denial is part of the psychological path to acceptance. People lie or over-exaggerate and you end up with all sorts of red herrings.
Lastly, I’d say we all have different levels of severity. If I were to say my symptoms a lot of people in the forum would be shocked. Acceptance, the body adapting and moving forward is easier if your condition isn’t extreme.
Out of all the full recovery stories I have read I think only a few rare ones actually tick the right boxes to satisfy certain issues or vibes I pick out from the stories. In most cases we also see only mild symptoms.
I think in many cases from the crash onwards other independent mechanisms in the body can likely adapt somewhat
It is likely. Some efforts probably have been made to offset the negative effects of epigenetic distortion to some extent in a patch-up manner, not at the level of the distorted gene, but at various levels above it. If that so, it itself is only an adaptation of body to our distorted genes. I am sure that it is very possible. Perhaps, thousands of up- and downregurated gene expression which is observed in researches may be rather the very such efforts.
My insomnia is as bad as yours…
Out of all the full recovery stories I have read I think only a few rare ones actually tick the right boxes to satisfy certain issues or vibes I pick out from the stories. In most cases we also see only mild symptoms.
On one hand, in many cases their symptom is mild enough that their recovery could be explained by such adaption.
On the other hand, generally speaking, epigenetic modofication is not irreversible in itself. And as you said there are rare cases which is difficult to explain their recovery only by limited adaption.
Whether the (probably epigenetically induced) AR-overexpression is (naturally) reversible or not is the critical issue.
If it is irreversible, why? Even if it is epigenetic and stubborn, it should return to normal with time, unless some factor(X) prevent it.
If it is reversible, we can definitely make some efforts as a kind of rehabilitation to encourage its slow recovery process.
What do you think about it. It is irreversible modification?
We don’t know what factor is preventing reversal and even many decades of research has not found the reason for this in CRPC.
Dr Alfonso may find something. Analysing the full genome is a new approach.
In literature there are anomalies few and far between like we sometimes see on PH.
There are possibly non-natural ways in the future. Older HDACi drugs are no good but perhaps future more targeted ones may work.
I finished reading the article: Drug resistance in metastatic castration-resistant prostate cancer: an update…
Thank you for the introduction. This scientific knowledge is definitely important. It’s also extraordinarily high level, but we can understand the outline. What a destructive and disastrous state of affairs. It seems impossible to correct these distortions.
However, all events and alterations which happen under anti-androgen therapy are really rational in themselves. Yes, our body, life system is not irrational.
In the end, as for scientific research and development of treatment, we’ll just have to leave it up to the scientists. But, I wanna believe our body’s wise and potential to re-regulate itself. Is there any idea to encourage the body’s self-repair…?
Anyway, thank you for your instruction.
Best regards
To your third bullet point, I have a couple of questions.
Firstly, why do people have different levels of severity. Why isn’t it standardised as the drug is having the same mechanism of action for everyone (I accept its effectiveness can mean people from 1 pill or 1000 can have crazy bad symptoms in developing PFS)
Secondly assuming we all agree this gene silencing or expression change is it as simple as to say those with more symptoms thus severity have more genes affected than those who are very very mild PFS case (if such a thing exists)
Or maybe EVERYONE with PFS has all these genes affected but the predispositions in our genetic make up result in how mild or severe the symptoms are