It would be great to have the lead scientists participate in Reddit ask me anything.
It would comfort sufferers and unite us with better most current knowledge.
What does everyone else think?
Can we put this forward?

It would be great to have the lead scientists participate in Reddit ask me anything.
It would comfort sufferers and unite us with better most current knowledge.
What does everyone else think?
Can we put this forward?
Great suggestion @Tyr would be a fantastic opportunity, positives to be had as you so rightly point out.
May even have a positive effect on donations with greater and wider interest
I don’t think they know anything yet.
The lead for PFS network study is a CRPC scientist and so will have better resources / knowledge than us from his areas. The theory is that the mechanisms are the same.
I’m sure a lot of people have questions and/or want to understand a little more. I personally have a few that are specific to his area of research.
Just like awor predicted 15 years ago…it would be the opposite of crpc but a similar mechanism instead of becoming super sensitive to androgens once deprived of we have become super insensitive to them and even a toxic gain of functioning once you increase it…
Yeah so that’s the same reaction to androgens as would be within CRPC. Super sensitive to the point of being insensitive / intolerant.
I hope that he could bring some light to such a bleak situation. 5+ decades haven’t cured it and there are still many different ways to fix the issue in theory… I wonder what his thoughts are on some of them with PFS in mind e.g. PARP inhibitors (if related genes suggest them), HDACi, AR vaccines perhaps in the future, other drugs that can suppress intracellular androgen levels etc etc.
Be nice to understand some of his thinking even if noon much of it can yet be anything but speculative. The speculative info and his ideal hopes would probably feel more reassuring than any of the hard facts.
I know it would be so nice to hear opinions on this…in theory if u could reduce androgen to extremely low levels it should provide relief.
I think the protein itself has changed, misshapen perhaps…didn’t someone hint at this earlier from talking to melcangi in private?
I dont know enough to speculate on it really but remember awor saying this back in the day from talking to multiple scientists in different fields including ar specialists and cancer researchers…
I castrated myself with estrodiol to treat this condition and it helps amazingly well as expected. Unfortunately even with castration and Estradiol I can tell I’ve got PFS and this is the mechanism.
It is obvious to me I am hyper-androgen like and periods where I achieve more feminine effects with estrodiol aren’t long lasting.
The AR tissues in PFS win in the competition between ER and AR. It’s frustrating because at times when I achieve periods of femininity via increasing E2 even more or shortly after a one time blast of androgen (decreasing AR as per Biplolar Androgen Therapy method) I feel on top of the world (not because of how I look but because the core symptoms of PFS totally vanish).
Worsening occurs when the shitty overexpression of AR appears again and I can see even ER effects decreasing.
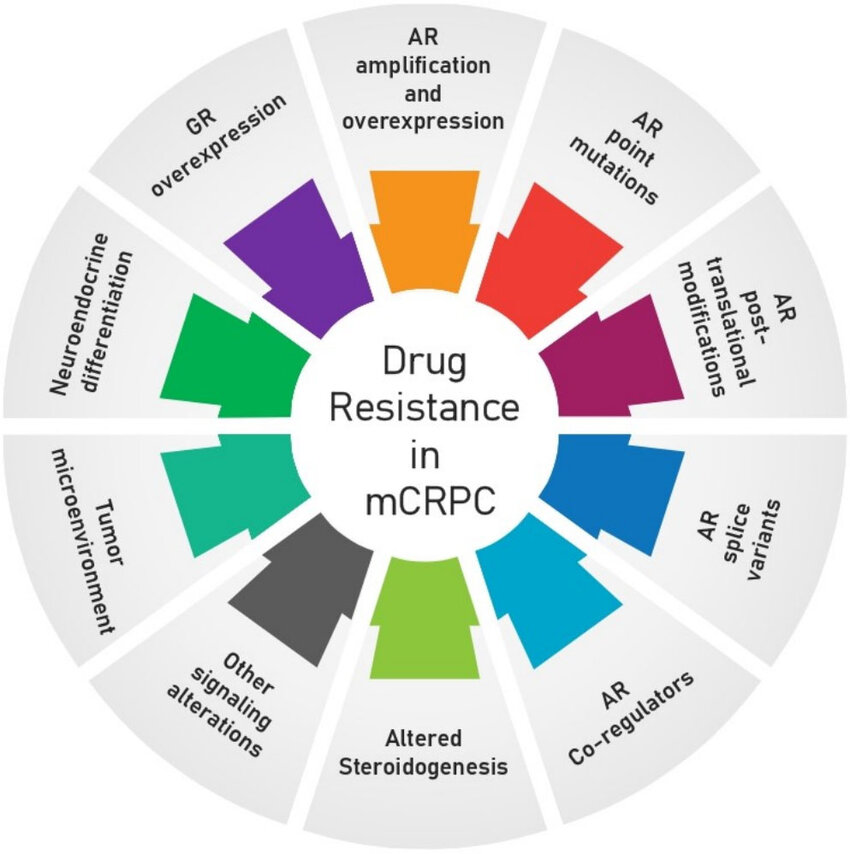
There are a few components. I’ll add a diagram to show.
I really would benefit mentally from experts speculating. There is plenty of info I know from my own reading but the lack of much expert talk is extremely hard and I read nobody else say much about it tbh. You mention some things now which is very nice to read and makes me feel less alone in the understanding of the condition. It shouldn’t be that way… we all should know equally and discuss.
From my own perspective if there was further treatment that could help but also would feminise me I’d be more than happy with that. So I wonder if there is something out there for my situation even if not for everyone else e.g. AR degraders, other methods to reduce intracellular androgen levels etc… if you can think of anything or speculate please do 
One I had in mind was trying abiraterone in my case. I’d be worried about long term consequences though without a scientists input. I wonder if low dose would prevent developing resistance.
Yes…we feel totally isolated and alone as if genetic freaks.
I dont think awor will ever post here again tbh…axo has also disengaged but I believe he was very physically ill as myself and many others are past the point of getting around anymore…
His? Isn’t Nadine Hornig the lead investigator?
Good point. They are both leads but for different studies.
Dr Alfonso who is leading the genetics study has the most solid hypothesis in mind. I’d especially like to hear from him… and any other academic who would be willing to speculate especially with CRPC mechanisms in mind. Reason is at the end of the day I just want out asap and I know this is the mechanism.
Dr Nadine is especially interested in epigenetics and this field happens to be one component found in the CRPC mechanism anyway.
It would help a lot of us mentally if any of these people would be willing to do an AMA.
I was leaning more towards Dr Hornig…Remember she’s and androgen receptor expert and the most likely cause is epigenetic changes that prevents it from reverting back…Or that is my understanding and Dr. Alfonso looking for a predisposition in genetics…What if there is no pre disposing genetic factor? Remember this is not a condition that occurs naturally in anyone and anyone with a endocrine system may be susceptible to it…Who knows???
All the more reason for discussion right!
Also I would like to add we have no idea a percentage of people who develop this…I’ve heard all kinds of percentages from less than 1 to over 10 percent…Also something with the original trials is off…It doesn’t add up have we’ve seen an explosion of pfs in the last 5 years or so…
Also didn’t someone conduct a smaller trial? Seems I remember reading they did and about 40 percent or more reported side effects even if it wasn’t pfs…but on drug side effects…Mercks clinical trial data doesn’t add up…with real world reports of what we are seeing today
I’d imagine he’s assuming he would see the obvious link that also makes CRPC genetically more likely. It’s stuff we already know so it will be gene repair genes that stand out and there might be other data he can find. It’s not necessarily anything more than a prediction of higher probability and also how we might respond to potential treatments. I suppose ideally we’d somehow genetically suppress genes that produce / initiate AR variants that have unique responses to hormones. It’s the necessary research for us right now to move forward. We would at least understand if PARP inhibitors are likely to help from this as an initial actionable step. Getting this prescribed might be hard.
PFS fits too closely with CRPC to be just epigenetic. I’ve done my own trials and reading purposely to prove this. Cba in going over it all again but if you want to chase purely epigenetic it’s leading no where unless some epigenetic modulating drugs work for CRPC.
Then the same will work for PFS. Pan HDACi don’t work; maybe HDAC6 inhibitors will. If any of these work I’ll be diy curing myself.
And no at this point I actually dislike discussion around other areas of “what it could be” because of how certain it is and therefore how much wasted resources will be spent elsewhere. Epigenetic yes but that’s not all components. It’s just an easy answer to say epigenetics.
In theory with CRPC epigenetic modulating drugs can fix the issue but in practice it’s hard and unlikely due to toxicities / off target effects.
Very interesting  I participated in Dr Alfonso study submitting a blood sample late last year…
I participated in Dr Alfonso study submitting a blood sample late last year…
Well I wonder then…How many men develop CRPC each year? Seems that would give us an idea atleast of just how many men have the genes to “possibly” develop pfs if exposed to finasteride…Its very complicated and the concepts are vague at this point but I like converse on here for a change…
For us it doesn’t matter how likely PFS is to develop. I don’t care at all tbh, however the likelihood will be different between finasteride and say a leading anti-androgen drug, the later being much more likely.
They can develop a genetic risk profile as done in CRPC and some signs will point towards treatment working. At current they use PARP inhibitors.
It might be vague but that’s also the same with CRPC gene research as far as I can tell. We want to put ourselves in a position to be suitable to any potential new treatments found within the next few decades.
IF say in the future CRPC is treated successfully in trials with new epigenetic drugs then we are very lucky and can make use of the epigenetic research.
This isn’t true.
All this seems overly complicated and there are way too many made up linkages between your hypotheses in cause / effect. It’s not realistic.
Also reducing AR expression seems to not usually be enough. We need to fix the issue further upstream whether that be somehow by destroying mutations, epigenetic mechanism or some other way.
Why remake the wheel when all the science is laid out for us in mCRPC literature.
PFS is the same mechanism as CRPC.
Cba in nitpicking each point. It’s cowboy scientists that have created crazy theories / protocols and waste everyone’s time in the past; I’m getting the vibes from you tbh. If not the case maybe you are too well read in certain areas and missing out major parts.
This topic was to discuss everything related to the idea of seeing if the scientists would be willing to do AMA…one is a prostate cancer researcher; the other is an androgen receptor researcher.
I don’t know if you watched Mitch’s interview with Hornig but she seemed reluctant to speculate beyond ‘we will gather data and see what it tells us’. I think that’s the right approach but probably not Reddit AMA material.
Fair enough with regard to her. I had the same thoughts when watching her.
It’s not the stance Dr Alfonso has. He has hypothesis of it being the same mechanism and that’s also my strong stance.
It’s good we have gotten both of them from different angles but Dr Alfonso is more onto something with this one. I’d imagine the AR researcher is just saying what she is aware of from her area of research and the limited PFS studies; whereas Dr Alfonso is more aware of anti-androgen use -> atypical reaction and all the unique signs of this (which PFS matches).
If Dr Alfonso is right and that is an extremely high probability to the point of verging on fact, then there are so many questions from there.