Hey @Fighter1, I’ll try to make a post but I don’t know if it will be helpful as everything except prolactin is technically “in range” and we don’t have much knowledge about what’s causing our issues.
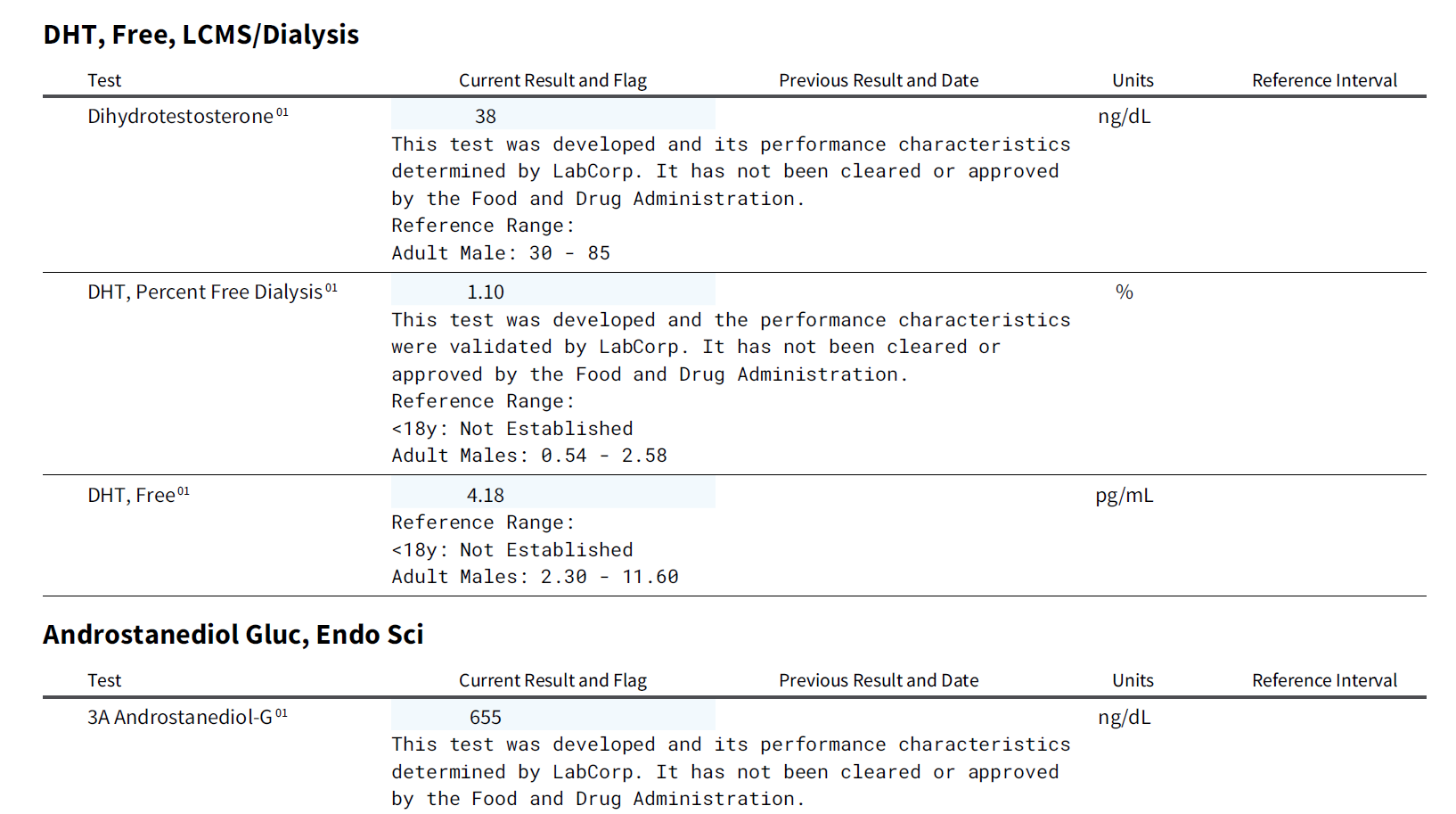
So to start with your DHT and 3a-diol g they’re all within range, but on the lower 1/3 of the range.
However it’s really hard to assess this values without before blood since they’re all very poorly understood.
It’s been shown that DHT levels indeed is very important for men.
This basically says that when T is above 350 ng/dL, DHT will matter more when it comes to having less symptoms according to AMS (aging male symptoms). If T is under 350 ng/dL it’s more important than DHT.
Since your T was around 650 ng/dL last time you checked, and if we assume it’s the same now, that would mean your T to DHT ratio is almost 6%, which is considered normal. But again on the lower side of things (normal 5-10% in serum).
I don’t see your SHBG anywhere but I’d guess it’s on the higher side since your last lab showed lower range free + weakly bound T and this lab shows lower range free DHT.
This is not uncommon in PFS, even though not everyone show this hormone profile either.
This article linked high SHBG to feminization of men with liver cirrhosis.
It’s not stated in the abstract but I downloaded the full article and controls had a SHBG of 25 nmol/L, while the liver patients had 50 nmol/L on average. On the other hand my SHBG was 23 nmol/L and I still have PFS so it can’t be the sole reason.
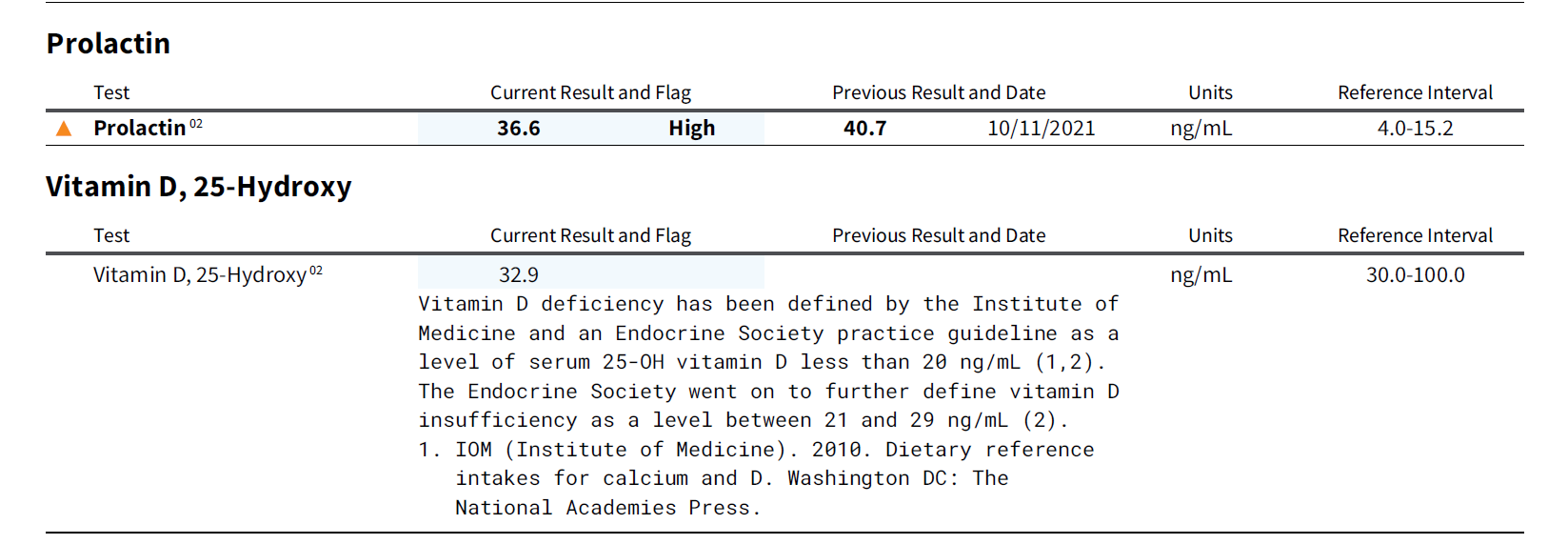
Your vitamin D is totally fine, 30+ is from my understanding sufficient (maybe even optimal). [The experts disagree somewhat, but around 30 ng/dL should be enough to not cause trouble.](https://www.health.harvard.edu/blog/vitamin-d-whats-right-level-2016121910893
High prolactin, probably is due to either low dopaminergic activity or not enough androgenic activity in the pituitary.
Maybe even a mix of both, as we know from rat studies that fin indeed dull the dopaminergic system, and we know from human studies that low DHT in CSF is pretty much uniform between PFS cases.
Would a dopamine agonist help? Maybe.
If it does indeed help, the conclusion would probably be that there’s enough dopamine receptors, but maybe downregulated dopamine synthesis is the cause. Estrogens are very protective of the dopaminergic neurons and estradiol is linked to alcohol consumption due to increase in dopamine, and alcohol consumption is decreased in PFS. Could be totally unrelated though, just an observation I made.
I’m guessing you will do the scan now and decide what to do after? Many people have had high prolactin and the trend is that it usually goes back to baseline after some time, but something like Cabergoline might speed up the process. You’ll need a very, very small dose and the side effects seems rare in these cases. But be careful and make sure your doc know what he’s doing if you chose this path.
Prolactin has indeed been linked to low libido.
But this is worth noting:
-
None of these patients with a high PL level had a pituitary pathology and 5 of these 16 patients had a low tT (31.3%).
-
only 42 patients had decreased libido and none of them had any type of endocrinopathy. Moreover, most of these patients had normal values of tT (80.5%) and PL (76%).
So it’s indeed also possible to have normal prolactin and still have libido issues. Yours are obviously way higher than the participants in this study (avg low libido 16.5 ng/mL, avg normal libido 10 ng/mL).
When it comes to E2 I note that it’s on the lower side of things. Actually your T and E2 almost match my own. I would be very careful about doing anything to lower it.
This is a interesting read about ED and E2/T ratios.
They noticed how T/E2 ratio can influence how one’s penis behaves, as presented in this diagram…
As you can see the group with the least E2 suffered from delayed ejaculation (numb penis anyone)? Just to give you an idea your value would be about 3.20, to get the same ratio that the control group had you’d need to raise your E2 to about 38 pg/mL if your T is stable.
Estrogens are indeed very important for male libido.
-
“What will surprise many people is that loss of sexual desire in men with low testosterone is due to lack of estrogen," Finkelstein said. “People think estrogen in men makes them very effeminate; they think of it as a female hormone, they think it is testosterone that gives men their sexual desire."
-
“It is amazing what we don’t know," said Finkelstein. “Even the most basic things we don’t understand about this drug that has been around for almost 80 years."
This are some good quotes from the article, and I totally agree with him. We have very little understanding on how things actually work.
It’s not uncommon that people get less sex drive with TRT (without PFS) for example. Even though some people think more T = more sexual appetite, it’s not really the case.
-
They found that the administration of testosterone with and without aromatase inhibitors markedly impaired sexual function when aromatization was inhibited.
-
Ramasamy et al. in 2014 showed that libido was increased in men receiving TST when testosterone levels were >300 ng dl-1 and estradiol levels were >5 ng dl-1. Most compelling is the fact that in men with serum testosterone <300 ng dl-1, sexual drive was seen to be markedly higher when estradiol levels were >5 ng dl-1.
5 ng/dL equals 50 pg/mL. In addition, when patients with low testosterone were treated with letrozole, a potent aromatase inhibitor, libido was decreased, suggesting that complete elimination of estradiol and decreasing the T/E ratio too severely, adversely affects sexual desire in men.
I don’t know why, but for some men it seems like finasteride actually decrease their E2 for some reason. This is a good case study, on someone who got blood while on fin.
If you read through the thread you’ll notice how his T plummets and his E2 follows. At some point he have <10 pg/mL E2.
This is while on the drug. While the general consensus is that total T and E2 should raise while taking fin, as you can see it’s not always the case.
I have no theory on why this would happen, but it is interesting nevertheless. In my own experience, lowering E2 is really bad for me. Muscle loss, aching joints and tendons with diminishing sensitivity in penis was my experience. Oh and also very, very dry skin + pain in hands while holding onto stuff.
I have no idea what to do about all these issues, but one thing is painfully clear and that is that decreasing enzyme activity is way easier than to increase it. Which is unfortunate because the metabolites of T is more important than T itself.
Also fin can change receptor density and it seems to not be only AR, but ERs as well. And without receptors, you could have all the hormones in the world and it wouldn’t do anything. On the other hand, if you have to high density it’s also bad. Very complex and can’t be measured very easily. Some hormones also regulate the expression of other hormone receptors. For example estrogen regulate progesterone receptor expression and progesterone regulate estrogen receptor expression.
I hope you got something out of this post, although it’s not much help when it comes to understanding PFS or deciding what treatment to pursue. Just some of my observations/thoughts on the matter.



 .
.