February 2018 Volume 15, Issue 2, Supplement 1, Page S81
Novel Penile Ultrasound Technique to Explain Mechanism of Erectile Dysfunction (ED) in Young Patients using Finasteride for Androgenic Alopecia
R. Rubin, A. Winter, I. Goldstein
PlumX Metrics
DOI: https://doi.org/10.1016/j.jsxm.2017.11.194
Oblectives: Post-finasteride syndrome (PFS), has been reported in young men with persistent sexual/non-sexual symptoms despite stopping finasteride prescribed for androgenic alopecia. Since these men typically have normal penile Doppler hemodynamics they are often diagnosed as having psychogenic ED. Animal studies, however, reveal histologic erectile tissue fibrosis after exposure to finasteride. Novel penile ultrasound techniques were used to assess if a similar pathophysiology could explain the ED in young men with PFS.
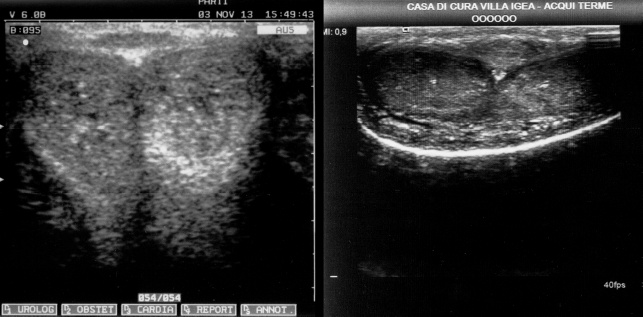
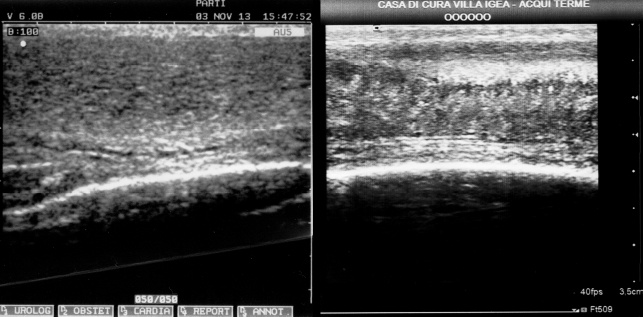
Material and Methods: 27 men with PFS (mean age 31 years) met inclusion/exclusion criteria: potent prior to but ED since use of finasteride; <40 years old without obvious cardiovascular risk factors; underwent grayscale and color penile duplex Doppler ultrasound with a high frequency probe (Aixplorer 15.4 MHz transducer) during maximal pharmacologic erection. Grayscale imaging was performed using a standard protocol in axial B-mode at multiple gains, with various dynamic ranges, in multiple penile shaft locations to determine presence/absence of erectile tissue homogeneity or heterogeneity. Standard color Doppler parameters of peak systolic velocity (PSV) and end-diastolic velocity (EDV) were concomitantly assessed.
Results: Mean use of finasteride was 3.5 years (range 2 days–12 years). PFS symptoms included ED (100%); IIEF, EF domain scores were on average 14 (range 0–24). Other PFS symptoms included low libido (81%), orgasm dysfunction (66%), cognitive changes (55%), and mood changes (74%). Dihydrotestosterone (DHT) blood test values were low/lower tertile in 56%. 26/27 finasteride users (96%) demonstrated lack of homogeneity and hyperechoic/hypoechoic regions in erectile tissue. One patient (4%) had homogenous erectile tissue. Mean right/left PSV values were 30.3/29.8 cm/sec, with mean right/left EDV values 1.6/1.1 cm/sec during maximal pharmacologic smooth muscle relaxation.
Conclusions: Using novel ultrasound technology, 96% of men with PFS and ED demonstrated heterogeneity in their corporal tissue at maximal pharmacologic erection. This new protocol is able to show that PFS men complaining of ED may have an underlying biologic pathophysiology. Further we hypothesise that finasteride lowers DHT leading to corporal smooth muscle apoptosis and fibrosis similar to animal models, impairing tissue expandability leading to clinically reported venoocclusive dysfunction and ED
Disclosure: Work supported by industry: no. The presenter or any of the authors act as a consultant, employee (part time or full time) or shareholder of an industry.