723 pages, 18k replies on repairing the long term damage from Accutane.
So many posts have been deleted, im seeing what I can find.
This was the member the had the lumbar puncture, I cant even click on his posts, they’re gone.
Jorcruz24 replied to IndigoRush’s topic in Prescription acne medications
So after about a year going from countless doctor to doctor, all the blood tests at least twice, MRIs, CT scans, lumbar puncture, I’ve been diagnosed with the following: -Fibromyalgia -Major Depressive Disorder -Irritable Bowel Syndrome -Sebhorric Dermatitis Im currently taking Zoloft and Wellbutrin, both antidepressants, and Cyclobenzaprine (muscle relaxant). As as far as self-care, I eat a relatively healthy diet, CBD/THC oil…
I just got my results from my Lumbar Puncture procedure and luckily (or perhaps unluckily) they did not find anything wrong with the cerebrospinal fluids. It’s at least some peace of mind, but back at zero—especially considering the fact the procedure caused leakage days later and I needed to go back to the ER to get a blood patch to seal it up (not fun!). I have a follow-up appointment with my neurologist on Monday, but over the phone he did mention tre possibility of…
From Babis,
After a visit to Mayo clinic, a few pituitary hormone tests, and pituitary stimulation tests, I finally confirmed the source of the problem.
It is hypopituitarism. My MRI showed a relatively small pituitary to begin with, but I never had problems because it was producing enough hormones.
However, when I took Accutane, it caused most pituitary hormones to drop to low or low-normal levels. After Accutane, I had low TSH, low FSH, and low IGF-1. I also had the testosterone of a 90 year old male, with inappropriately normal LH. If testosterone is low, LH should not be normal; the pituitary should elevate LH to signal the testis to produce more testosterone. If it doesn’t, then the pituitary (or hypothalamus) is not working properly. This is called hypogonadotrophic hypogonadism.
The articles I have posted above confirm that Accutane lowers pituitary hormones. In addition, my hypogonadal symptoms occured acutely while on Accutane and partialy diminished once stopping, so there is little doubt left that accutane causes hypopituitarism to susceptible individuals. What is not mentioned in the literature is that the damage may be permanent or long-term. If it causes apoptosis in sebaceous and meibomian gland cells, what would stop it from causing apoptosis in other glands as well, such as the pituitary gland?
When Crisler said in an interview that US endocrinologists know zilch about hormones, I was skeptical but, sadly, I found out the hard way how right he was. Yes, on lab reports, most of my hormone levels looked “normal”, i.e. within lab range, so most endocrinologists thought my hormones were fine. Some of them suggested viagra or a penile implant (!) although I am only 33 years old. 8 out of 10 endocrinologists are not open to the fact that “normal” levels should be age-adjusted. You cannot consider the testosterone level of a 90 year old male normal for a 30 year old male. They were also happy that my LH was normal, and unable to recognize that it was inappropriately normal. It was only Alan Jacobs (neuroendocrinologist in NY city) that recognized this as a sign of hypogonadotrophic hypogonadism. But the growth hormone deficiency (due to hypopituitarism) was missed for another year, until I asked my endo for an IGF-1 test and, once that was abnormally low, a GH stimulation test. The test showed a zero GH response of the pituitary to stimulation!
I had to read hundreds of medical journal articles and see >50 doctors of all specialties before ending up in the right experts, doing the right tests, and zero in on the right treatments.
Anyway, since I confirmed the source of the problem I focused on treating the underlying cause. One can replace the missing hormones, but it is much better to restore their natural production by the body. I read guidelines on testosterone replacement therapy (such as those of John Crisler) but had to tweak them to suit my needs. I am doing well on low dose HCG + low dose testosterone gel. The usides and downsides of this protocol are detailed in Crisler’s articles and interviews. Exogenous testosterone supressed natural production of testosterone by the testis, and LH & FSH by the pituitary. The upside of HCG is that it stimulates the testis to procuce testosterone naturaly, preventing testicular atrophy. However, it is still supressive to the pituitary. For this reason, I only take low doses that allow me to feel well but do not supress my pituitary too much. Moreover, to wake up my pituitary from time to time, I take a very low dose Clomid regimen for a week of every month or so. This stimulates the pituitary to produce LH and FSH. I feel much better in this regime, testis size has been restored (it was decreased for 1.5 years post-accutane) and muscle size is also beginning to be restored. Most importantly, I do not feel weak and exhausted like I did, and my heart pumps much better. I also found that Citicoline (an acetylchonine precursor) increases all pituitary hormones, which is perfect for me, and seems to have helped restore psychogenic erections (which were also lost for 1.5 years post-accutane). It increased my IGF-1 from 120 to 160, and I hope to increase it further to age-appropriate levels.
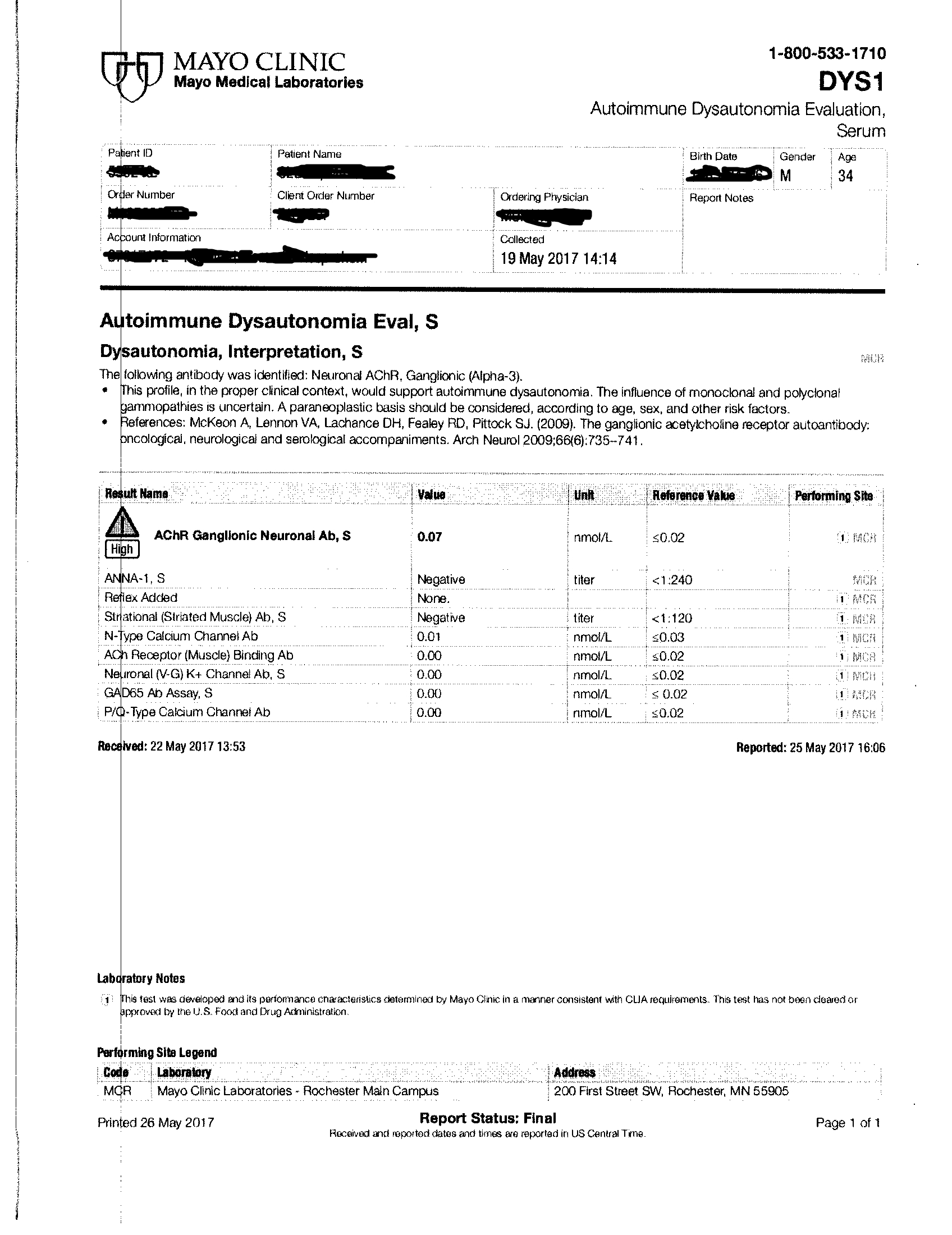
As I mentioned in other posts, I also developed autoimmune autonomic ganglionopathy after accutane. This is a potentially life-threatening autoimmune neuropathy mediated by neuronal acetylcholine receptor autoantibodies. The decreased number of alpha-3 acetylcholine receptors on my autonomic ganglia may be an extra reason why Citicoline helps me.
By the way, after 4 years of workup and every endocrinology test available, my official diagnosis is hypogonadotropic hypogonadism and subfertility secondary to partial hypothalamic insufficiency, due to isotretinoin treatment . I hope this helps other people with problems: find a good reproductive endocrinologist (don’t go to a generic endocrinologist, they are clueless) and get your hypothalamic function tested.
Well, I haven’t visited the website for ages and you probably do not need my reply anymore, but here are the articles again:
Evidence for decreased androgens, neurosteroids and their receptors:
Evidence for decreased androgen 5 alpha-reduction in skin and liver of men with severe acne after 13-cis-retinoic acid treatment.
J Clin Endocrinol Metab. 1994 May;78(5):1064-9.
Effect of oral isotretinoin treatment on skin androgen receptor levels in male acneic patients.
J Clin Endocrinol Metab. 1995 Apr;80(4):1158-61.
Excerpt: " The present study clearly demonstrated a decrease in androgen receptor binding capacity… The isotretinoin-receptor complex may interact with cis-acting response elements in the promoter region of regulated genes, repressing the gene transcription encoding for the androgen receptor, the gene transcription encoding for the 5-alpha-reductase activity, or both transcriptions simultaneously ."
Epigenetic side-effects of common pharmaceuticals: A potential new field in medicine and pharmacology.
Med Hypotheses. 2009 Nov;73(5):770-80.
Excerpt: " The following adverse effects have been reported to persist, even after discontinuing therapy, suggesting persistent (or perhaps slowly-reversing) gene expression changes and epigenetic effects: alopecia, arthralgias, ocular abnormalities, inflammatory bowel disease, keloids, osteopenia, hyperlipidemia, erectile dysfunction, and psychiatric disturbances. Isotretinoin is postulated to have complex effects on the brain and central nervous system. "
13-cis-retinoic acid competitively inhibits 3 alpha-hydroxysteroid oxidation by retinol dehydrogenase RoDH-4: a mechanism for its anti-androgenic effects in sebaceous glands?
Biochem Biophys Res Commun. 2003 Mar 28;303(1):273-8.
Isotretinoin, tetracycline and circulating hormones in acne.
Acta Derm Venereol. 1997 Sep;77(5):394-6.
Effects of isotretinoin on male reproductive system.
Lancet. 1994 Jul 16;344(8916):198.
Erectile dysfunction during isotretinoin therapy.
Actas Urol Esp. 2005 Nov-Dec;29(10):974-6.
Acitretin-associated erectile dysfunction: a case report.
Cases J. 2009; 2: 210.
In animals treated with retinoids, testicular atrophy with spermatogenetic arrest was described:
Toxicology, carcinogenicity, and teratogenicity of some orally administered retinoids.
J Am Acad Dermatol. 1982 Apr;6(4 Pt 2 Suppl):652-9.
Retinoid receptors involved in the effects of retinoic acid on rat testis development.
Biol Reprod. 2001 May;64(5):1307-14.
In humans treated with retinoids, pituitary hormones (including LH and FSH), testosterone and IGF-1 where suppressed:
Isotretinoin influences pituitary hormone levels in acne patients.
Acta Derm Venereol. 2011 Jan;91(1):31-4.
Effects of chronic retinoid administration on pituitary function.
J Endocrinol Invest. 2005 Dec;28(11):961-4.
Short-term isotretinoin treatment decreases insulin-like growth factor-1 and insulin-like growth factor binding protein-3 levels: does isotretinoin affect growth hormone physiology?
Br J Dermatol. 2010 Apr;162(4):798-802
13-Cis-retinoic acid decreases hypothalamic cell number in vitro.
Neurosci Res. 2010 Nov;68(3):185-90
By the way, after an LHRH stimulation test and a number of other tests, my endocrinologist finally narrowed down the problem and diagnosed me with partial hypothalamic insufficiency (leading to low testosterone, low growth hormone, and low cortisol). So I have hypothalamic hypogonadism. The fact that accutane damages the hypothalamus is confirmed by the last four papers in the above list. (Of course, 99% of endocrinologists have never heard of this literature because they never prescribe accutane - dermatologists do - and dermatologists do not read endocrine journals).