Guys, just wanna give you a brief update on what can happen, when tappering off Finasteride at 0.5 Micrograms per day (that’s a 2000th of a single pill!):
A few of you already know that I am tappering off Finasteride at micro dosages since more than a year. Before tappering off I mainly had severe sleeping problems and a little bit of sexual dysfunction. All kinds of symptoms became worse and I got the full spectrum of symptoms while reducing the medication. I have to add that during that time my sexual functions got down to 15-30%, but I didn’t experience complete impotence at any time. The neurological symptoms though were a nightmare, with me not sleeping more than 1h per day for six weeks at the worst time and around only 2-3 good hours for another 10 months. Things seem to slightly improve.
Once I dropped under 180 Micrograms funny things started to happen: I didn’t had mornimg erections for years and suddenly they came back. But not normal morning erections but painful, prolonged, stone-hard erections that lasted for hours or the whole night, making me waking up in again and again. This wouldnt be associated with any kind of pleasure or sexual desire. It would happen completely automatically.
This would go for a week or two. Then they would suddenly stop completely and I wouldn’t have any nightly erections for 2 months.
I made DHT tests twice: once the day they suddenly stopped: DHT was normal. Once during a period when I didn’t had any erections at all: DHT was completely down.
I started tappering off because I saw that as a possible opportunity to avoid lasting PFS. I read that most guys start to get symptoms when they stopped taking Finasteride. Without knowing much about the pathomechanism I theorized that stopping finasteride or taking it irregulary, may cause disinhibition of the 5ar-enzyme with an overshoot of DHT as a consequence (some guys wrote they felt a lot better for a short period of time after stopping Fin before they finally crashed). I further theorized that the unnaturally high spike of DHT (just theory) would trigger a feedback loop that finally would cause the irreversible symptoms (epigenetic changes in the brain and /or other tissues - > depending on whether these changes would be rather in the brain or rather in peripheral tissue that would explain the differences in methylation and symptoms among patients).
I threw a look at the crazy inhibition curve of Finasteride:
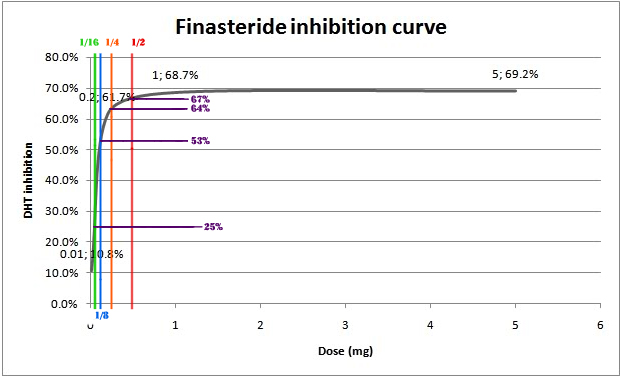
Based on that and now also on the heaviness of symptoms, I reduce Finasteride.
Since a year I feel I am crashing every second week, but it seems to get slowly better.
I am writing this post mainly because I want to point out that even 52 Micrograms per day (2x26mcg) still have certain effects on the body and that even a reduction of 0.5 mcg per day results in symptoms (hypererections) that are most likely be cause by feedback loops that kick in although I reduce it that slowly.
I just want to say, we should have a closer look on what the process of disinhibition does to the hormone and neurosteroide feedback loops in the body and specific tissue.
I propose
- testing various metabolites under the reduction of Finasteride at various points of time and dosage
- doing the same experiments with rats (also looking at several tissues)
- repeating these experiments under the use of body on a chip technology and brain on a chip technology, also using radio nucleotides to mark and trace finasteride during its binding and metabolism process.
Take care and cheers.
@axolotl @Dubya_B @anon22245532 @Sibelio