
Does anyone have advice for what I should talk about with my urologist? I have been referred to one who is familiar with PFS. Could I use any information in this thread to help him guide his hypothesis testing?
Methylation of a gene can be only in certain cells, not all cells of the body. That’s why every organ in your body is different despite they have the same genetics. So yes, there are PFS studies were methylation was seen in the cells of the brain liquid (that is difficult to get so I suppose there was no methylation in blood) cells. But I like the idea to check methylation in various tissues - it makes a lot of sense
Castrated rats have no testicles to produce TRT, but they do have fully functioning 5a-reducrase that turns TRT into DHT and other compounds. I think that’s the difference between us and castrated rats
5ar is not our problem. 5ar still work. Problem is the AR that doesn’t respond to the hormones.
5ar gene methylation seems to be at least accountable for the neurological symptoms. A healthy brain is also important for libido, erection, ejaculation and the regulation of sexual hormones.
I submitted a draft wikipedia article yesterday. If/when it is accepted I will post a new topic to the forum. It had extensive references to scientific papers including five meta-analyses.
Melcangi and colleagues in Italy are looking at neurosteroids. Here’s a new article that discusses neurosteroids. Warning that it is complex and speculative. See Section 1: Introduction and section 1.2.
Post-finasteride syndrome: An emerging clinical problem
Silvia Diviccaro, Roberto Cosimo Melcangi & SilviaGiatti
Neurobiology of Stress, vol. 12, May 2020
https://www.sciencedirect.com/science/article/pii/S235228951930061X
Thanks, you are doing a great job, man!
Another paper I came across yesterday that discusses neurosteroids:
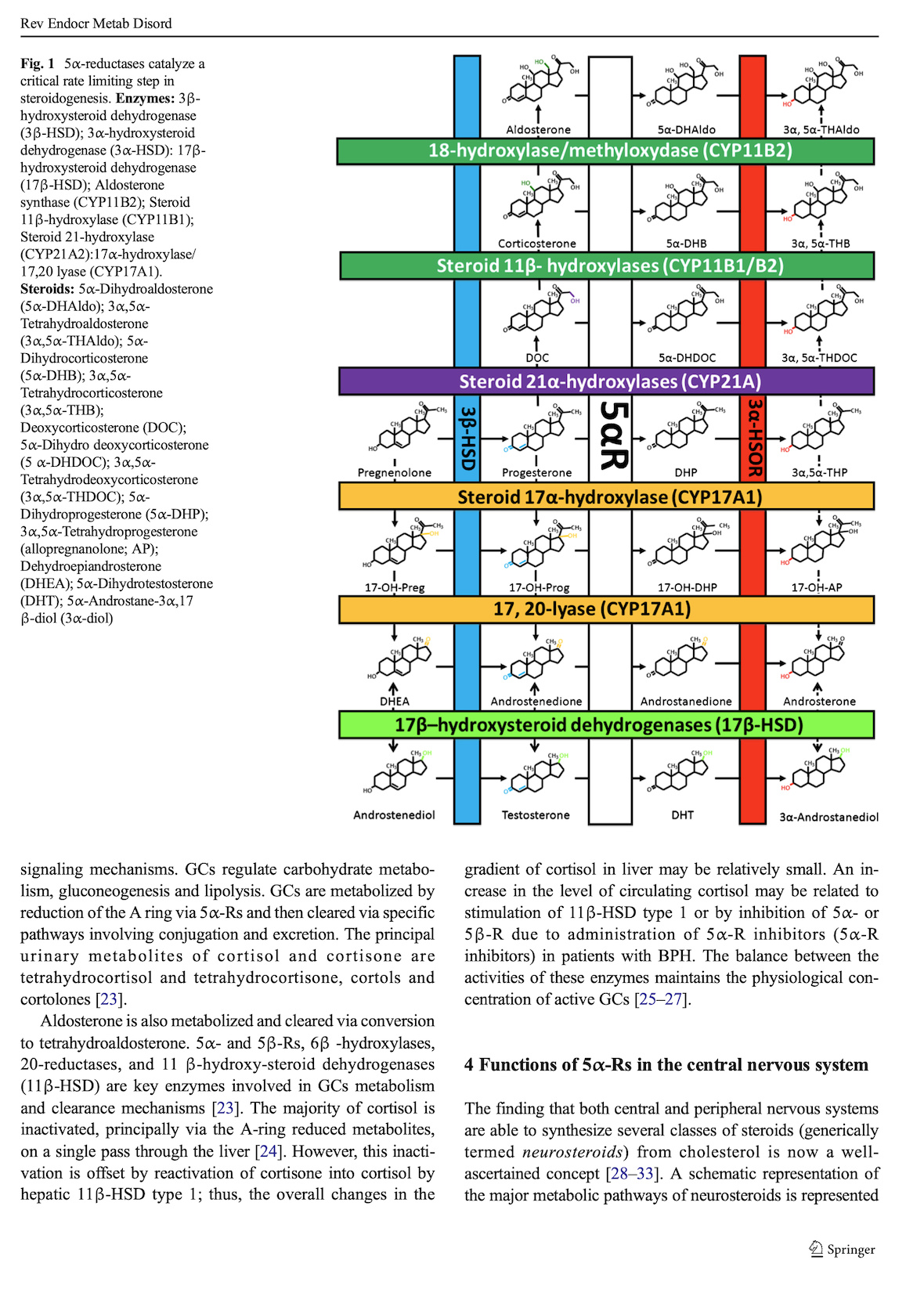
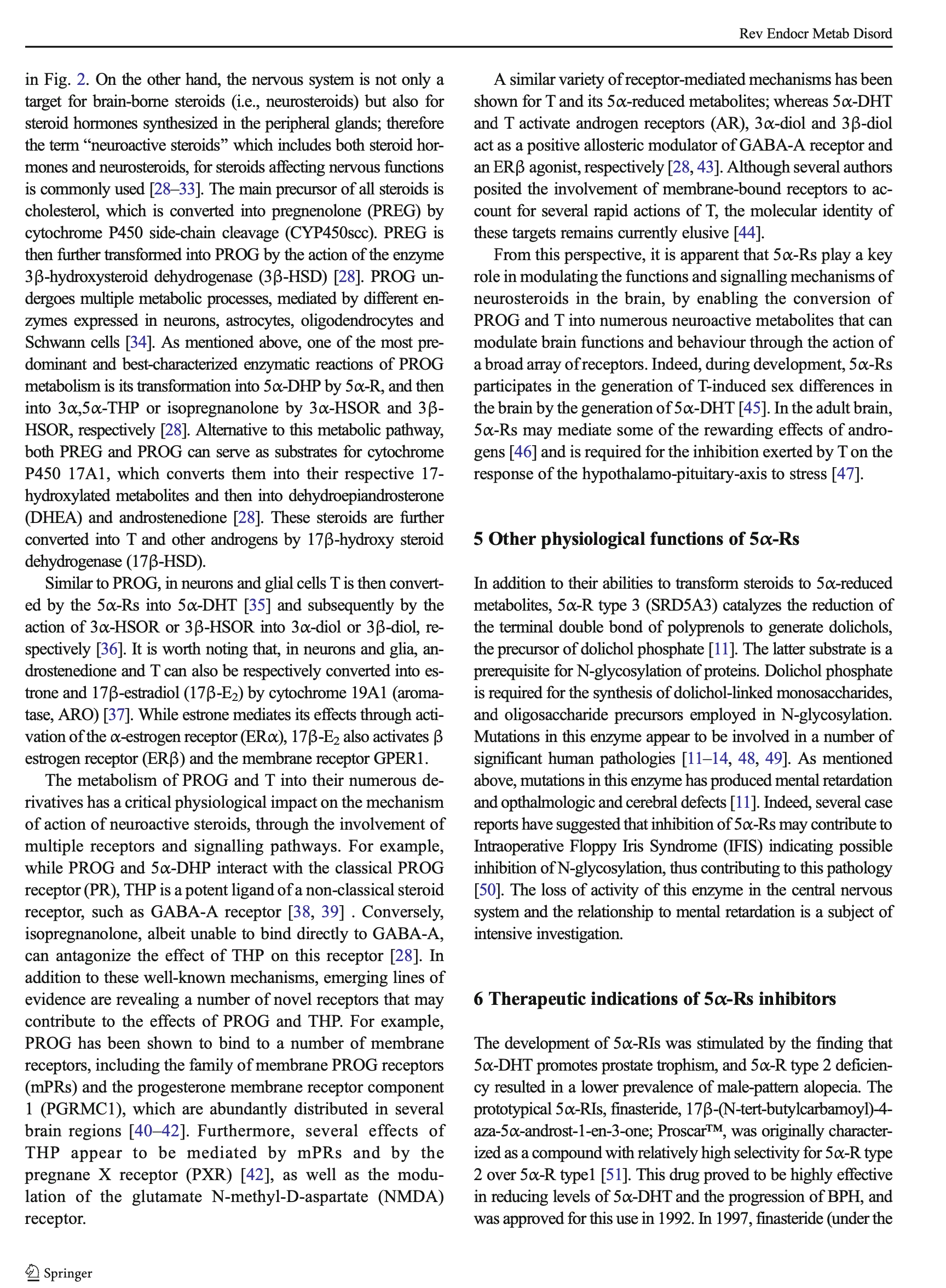
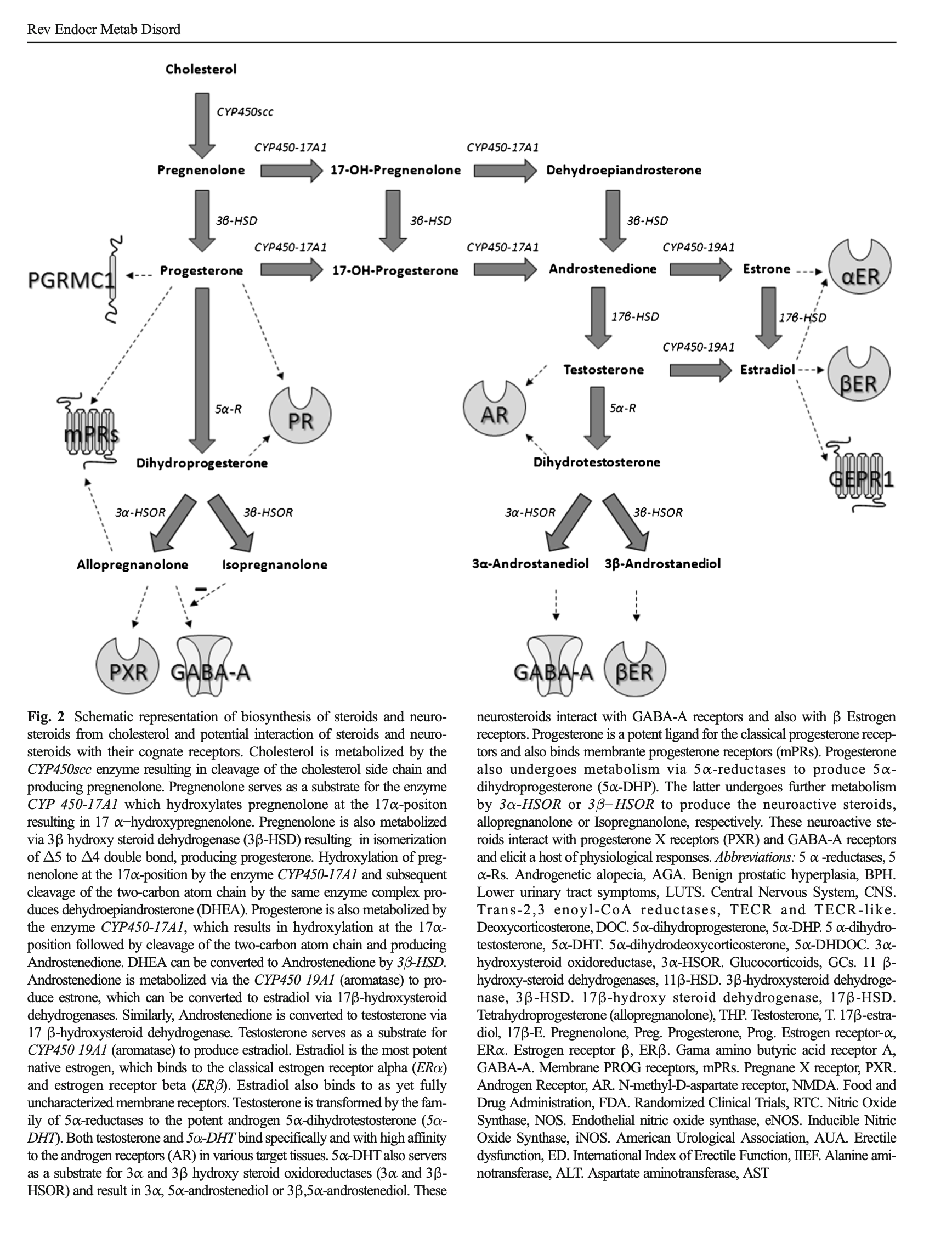
Adverse effects of 5α-reductase inhibitors: What do we know, don’t know, and need to know?
Rev Endocr Metab Disord
Traish AM, Melcangi RC, Bortolato M, Garcia-Segura LM, Zitzmann M
http://doi.org/10.1007/s11154-015-9319-y
https://www.ncbi.nlm.nih.gov/pubmed/26296373/
Attaching pages 1-5 as images (can’t upload PDF). Scihub has the full text. To find it, enter the DOI: 10.1007/s11154-015-9319-y
See especially Sections 1-5.


Unfortunately it does’t show the full article here.
I highly recommend this article to anyone who whats to understand PFS. It also explains really many of the other symptoms like neurological deficiencies, blurred vision, increased risk for diabetes, cancer, heart-disease, stress intolerance. 5ar could even explain pain and skin changes.
I find it highly concerning that blocking 5ar inhibitors lead to death of brain cells! I am highly convinced that future studies will show increased risk for Alzheimer’s and Parkinson’s for Finasteride users.
If you have problems to read the full article https://link.springer.com/article/10.1007%2Fs11154-015-9319-y, some people use sci-hub.se to get around the paywall. Probably legally gray.
Malfunctioning enzyme is most likely an inaccurate term. What I mean is disrupted 5ar2 enzyme function. This can in theory happen in more than one ways but the evidence points towards lack of gene expression of the gene encoding for 5ar2 (SRD5A2), which essentially means the enzyme is not produced in the affected cells.
At the tissue level, some cells may still be producing the enzyme, so the enzyme will not be completely absent from the tissue but will be highly reduced in concentration (and, in many people, more so than during regular Finasteride administration).
I have no idea how this specifically happens at the sub-cellular level or what all the different ways it could happen are but all evidence indicates, in my opinion, that it happens as a response to sufficiently low or rapidly falling DHT levels, which admittedly seems paradoxical.
The evidence in support of this theory is that people can get PFS from a single Finasteride pill, without any prior exposure. The reason I believe these reports is because I myself got PFS from a single pill. It happened within 20 minutes of taking the pill so there is no doubt it happened during a phase of falling DHT.
Note that this theory is in contravention to the dominant theory of PFS, which argues that genes are methylated in PFS as a response to rising DHT levels after cessation of Finasteride treatment in an environment of upregulated androgen receptor (AR) from prior finasteride use.
The dominant theory, in my opinion, cannot explain my experience and the experience of many others who got PFS from a single pill. It can also not explain, in my opinion, the experience of people who got PFS while they were on Finasteride.
The dominant theory can only explain, to my knowledge, the experience of people who get PFS only after stopping Finasteride. I believe, however, that this is a separate type of PFS (what I have dubbed PFS type 1), which is not caused by methylated genes (and is therefore less permanent) but by the state of AR upregulation coupled with an HPTA axis hormonal crash after stopping Finasteride. This, of course, is speculative.
Likewise, the dominant theory would predict that PFS can in theory be begotten from extremely high levels of androgens from steroid abuse when AR are overwhelmed, even without prior finasteride use or AR upregulation. This does not happen to my knowledge.
Thanks a lot. I heard from people who got PFS from a single pill, but I thought it is due to the irreversible binding to the enzyme, so that the enzyme receptor complex is slowly cleared from the blood, which itself could lead to rising DHT levels that silence the 5ar-gene in a feedback loop.
I also thought the the upregulation is just a sign, that DHT or following cascades are too low or not working anymore.
PFS within 20 minutes turns down most of the theories that made sense to me.
Because I heard people get PFS when they reduce finasteride and because of the dominant theory I decided to tapper of finasteride super slow: the first 800 mikrograms over 5 months and since 9 months I tapper down 0.5 micrograms a day.
Reaching 230 micrograms I crashed (while tappering off mirtazapine - probably I had the crash already 1 year before but could cover most symptoms with mirtazapine).
Another thing that I notice were morning errections came back in waves under 180 micrograms, but they were oftentimes so long and painful that I woke up from it (contrary to what one may think they were not coming with any pleasure or sexual desire, they were completely disconnected from my brain). These hyper errections took place until under 100 micrograms although I went down less then 0.5 sometimes just 0.3 micrograms a day! I am still tapering off (73 micrograms now in 2 daily doses). The insomnia and mental symptoms are hardly bearable. Sex life is rare and not connected to much pleasure.
I would also support that there are various types of PFS (I think it depends on which organs are most affected by the 5ar-silencing). Does your type of PFS include mental problems like insomnia? And what where the first symptoms you experienced after 20 minutes? Were they different from what you experienced after 4-6 weeks (full clearance of the finasteride-enzyme-complex)?
This is what my experience felt like as my mileage decreased and my weight increased while energy slowly decreased like clock work…As if something was slowly leaving your body month after month until you are just now left as an invalid slob…
Does finasteride affect the brain of everyone who takes it or only those who develop pfs?
Why does pfs then only happen to some people? Is it only some of us that that finasteride that it effects our brains?
It 100% affects everybody…I was always someone who dreams a lot, and very lively dreams, and it might seem stupid, but i had solved lots of my problems dreaming of solutions for them (Even maths problems, and im really not lying)…
I took that poison 3 years, during which i stopped dreaming all at once…I always thought, it must be im getting older, or too much stress at work, but boy i was wrong…3 years, and my libido and errections were intense like when puberty hit, and BAMMMMM everything is dead, 0 Libido, 0 errections…But at least im dreaming again now, so i know 100%, that it was that poison, that fucked up my brain
Are you still tapering off that and how long have you been on it? This by itself can lead to psychological and neurological side effects for years after you stop completely, depending on how long you were on it.
No, I was on mirtazapine for 1 year in varying doses and try to cut it several times.
The crush was actually following the last doses of mirtazapine. I was reducing finasteride the same time, so it is difficult to say what is causal. The symptoms fit to PFS as it is not just neurological. Mirtazapine is also changing some Neurosteroide and cortisol pathway, therefore my best guess is finasteride first caused insomnia and tension, taking and tapering mirtazapine worsened the symptoms to full blown PFS
The erections got first stronger when you stopped it?