
I wrote a very long post about this issue above. The DHT needs to be at high concentrations in certain tissues, which may be impossible to deliver through systemic administration, at least not without frying all other tissues. For example, DHT concentration in prostate is ten times higher than in serum.
1 Like
Ah I understand. What you’re saying is with no 5-ar you’re not going to be able to get the proviron/mast/tren to the tissues they need to go to since TRT needs to do it? Is that right? Sorry I’m dumb as fuck. If so That sucks.
However they should reach muscles, hair, brain and our dick right? Why would 25mg when I was natty on Proviron be constantly getting hard ons? Surely there is something to it?
Unless you’re telling me I can never have any DHT function again? Is that even a possibility? I was thinking my body just needs a strong DHT deriv to power the receptors since theres not much more 5-ar producing DHT and thats why my TRT is so weak.
Either way, in a few weeks we’ll known because I plan to run Proviron then Mast. I’m just hoping for an alpha male feel and libido again, thats all. I’m not trying to ‘cure’ things per se.
Put a plaster on PFS would be a better description. I’d run grams of this shit if it’d fix me. The worse case scenario is my body rejects the DHT derivs and I can’t use them. That would be a horrible future and life.
I guess it depends on what you mean by “deteriorate”. In other words, what exact symptoms of PFS become worse? Or are we also talking about new symptoms (which are in this case side effects of supplementation) that appear with such androgen supplementation?
In general, the body has arrived at a certain hormonal equilibrium even with a broken machinery. There are numerous feedback loops that aim to preserve that equilibrium. When you introduce an exogenous androgen, this equilibrium will be disrupted, and you are likely to feel worse as many hormones will be outside their normal ranges.
This would be especially so if testosterone and estradiol are in normal ranges to begin with as is the case with most people with PFS, especially PFS type 2, as I call it. Adding more testosterone will raise estradiol and a whole host of other hormones, which may result in side effects such as palpitations and headache, to name a few.
At the same time, the added androgens will not result in magnified androgen signal as in healthy people, due to lack of conversion to DHT. So you will not get a positive effect of rising DHT but you will get a negative effect of rising Estradiol. T/E ratio will be the same but the level of E will be higher without the opposing effect of higher DHT, and that may make things worse.
Similarly, if serum DHT is raised through supplementation, this may fool the body that 5a-reductase is functioning properly through negative feedback loops, which in turn will decrease precursor hormones such as progesterone and testosterone.
In this case, it is not clear what the total effect on tissues DHT will be but it is clear that tissue concentrations of 5a-DHP and allopregnanolone will fall, as progesterone will be lower. (My progesterone fell by 33% when I started supplementing DHT.) This may lead to some worsening symptoms.
As you can see there are lots of ways to account for feeling worse on androgen supplementation. Essentially, if the mechanism (DHT conversion) though which androgens exert most of their androgenic effect in the domain of PFS symptomatology (i.e. sexual function) is lost, all you are left with are the side effects of having hormones out of their normal ranges.
If TRT or any systemic hormonal manipulation were to work in alleviating symptoms of PFS, which might be partially possible but very difficult indeed with a fundamentally broken hormonal machinery such as malfunctioning 5ar, a compromise needs to be made essentially how the dysfunction will be allocated across the endocrine system and what side effects can be tolerated.
6 Likes
It’s a combination of new symptoms appearing and a worsening of existing symptoms. It’s as though exposure to androgens produces more symptoms that are associated with extremely low testosterone/DHT.
1 Like
Pls keep us updated 
1 Like
I have a thread I’ll be updating as a log. Keep yourself posted for updates 
My case exactly.
@Sibelio I’m very much following your theory and explanation. You seem to be constantly steering people back towards the underlying issue of a ‘malfunctioning’ AR, which does seem to fit with most all our symptoms and reactions to protocols.
Do you (or anyone else) have theories on how exactly taking FIN would leave some with a malfunctioning enzyme?
Epigenetic changes I somewhat comprehend, but don’t understand the full mechanism by how the drug would cause an epigenetic change in the formulation of an enzyme, leaving it malfunctioning. Otherwise, are there any other theories that could present how our conversion mechanism (the enzyme) would be malfunctioning, besides epigenetic?
1 Like
Do you know whatever happened with Mew? I guess his theory was along these lines about a decade ago. I wonder if he is still around and optimistic about prospects for recovery.
2 Likes
Does anyone have advice for what I should talk about with my urologist? I have been referred to one who is familiar with PFS. Could I use any information in this thread to help him guide his hypothesis testing?
Methylation of a gene can be only in certain cells, not all cells of the body. That’s why every organ in your body is different despite they have the same genetics. So yes, there are PFS studies were methylation was seen in the cells of the brain liquid (that is difficult to get so I suppose there was no methylation in blood) cells. But I like the idea to check methylation in various tissues - it makes a lot of sense
1 Like
Castrated rats have no testicles to produce TRT, but they do have fully functioning 5a-reducrase that turns TRT into DHT and other compounds. I think that’s the difference between us and castrated rats
1 Like
5ar is not our problem. 5ar still work. Problem is the AR that doesn’t respond to the hormones.
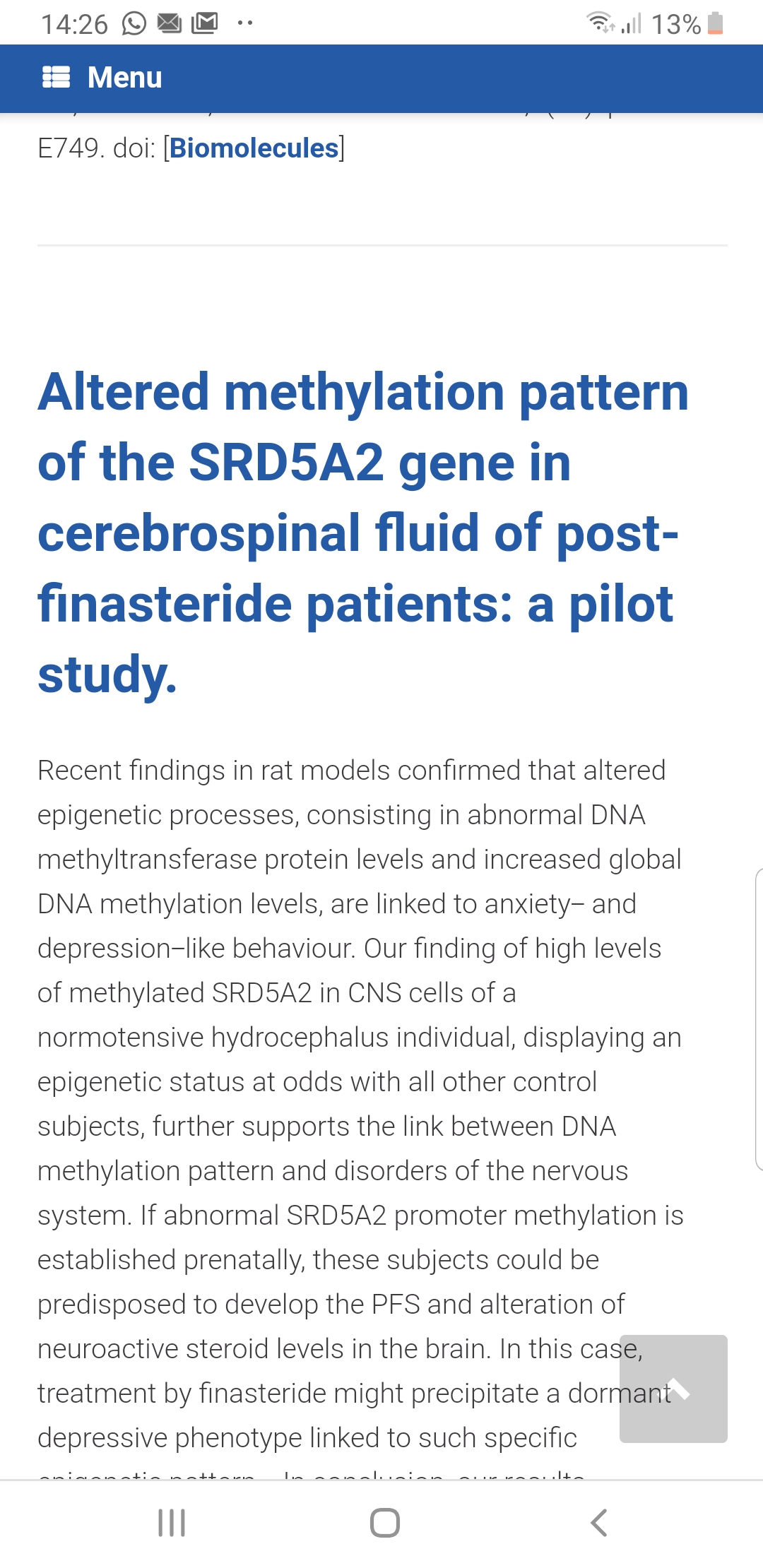
5ar gene methylation seems to be at least accountable for the neurological symptoms. A healthy brain is also important for libido, erection, ejaculation and the regulation of sexual hormones.
I submitted a draft wikipedia article yesterday. If/when it is accepted I will post a new topic to the forum. It had extensive references to scientific papers including five meta-analyses.
1 Like
Melcangi and colleagues in Italy are looking at neurosteroids. Here’s a new article that discusses neurosteroids. Warning that it is complex and speculative. See Section 1: Introduction and section 1.2.
Post-finasteride syndrome: An emerging clinical problem
Silvia Diviccaro, Roberto Cosimo Melcangi & SilviaGiatti
Neurobiology of Stress, vol. 12, May 2020
https://www.sciencedirect.com/science/article/pii/S235228951930061X
1 Like
Thanks, you are doing a great job, man!
1 Like
Another paper I came across yesterday that discusses neurosteroids:
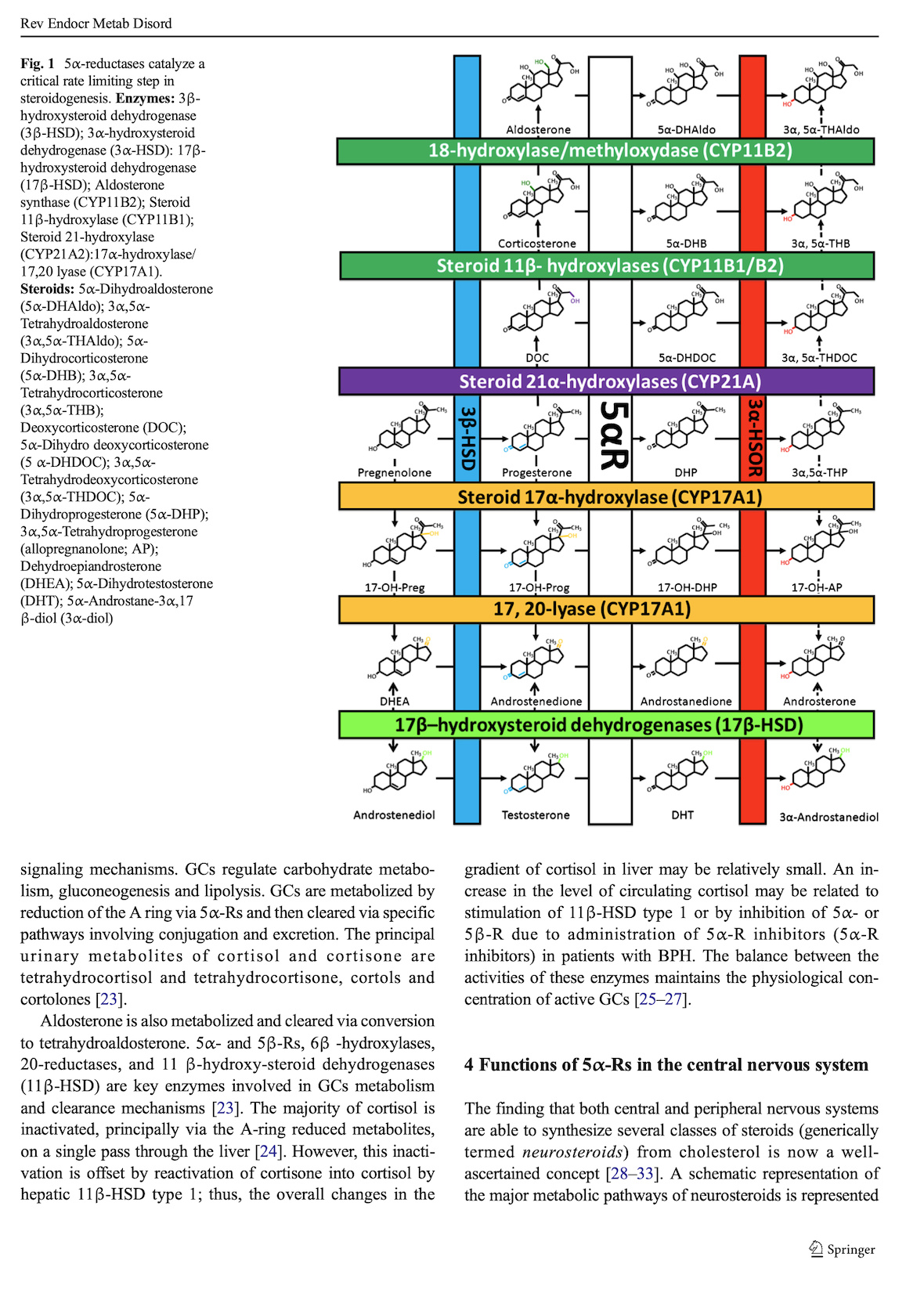
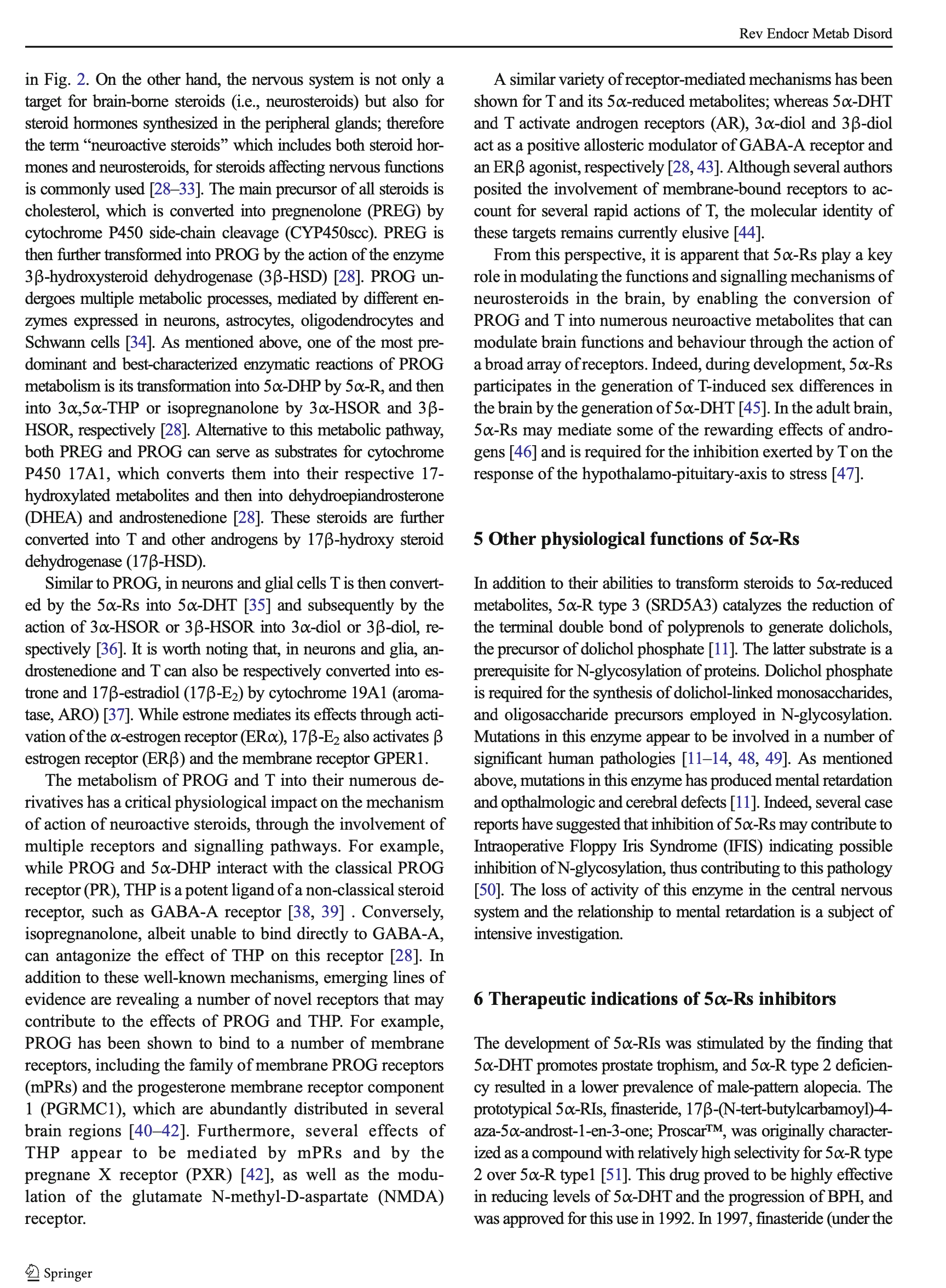
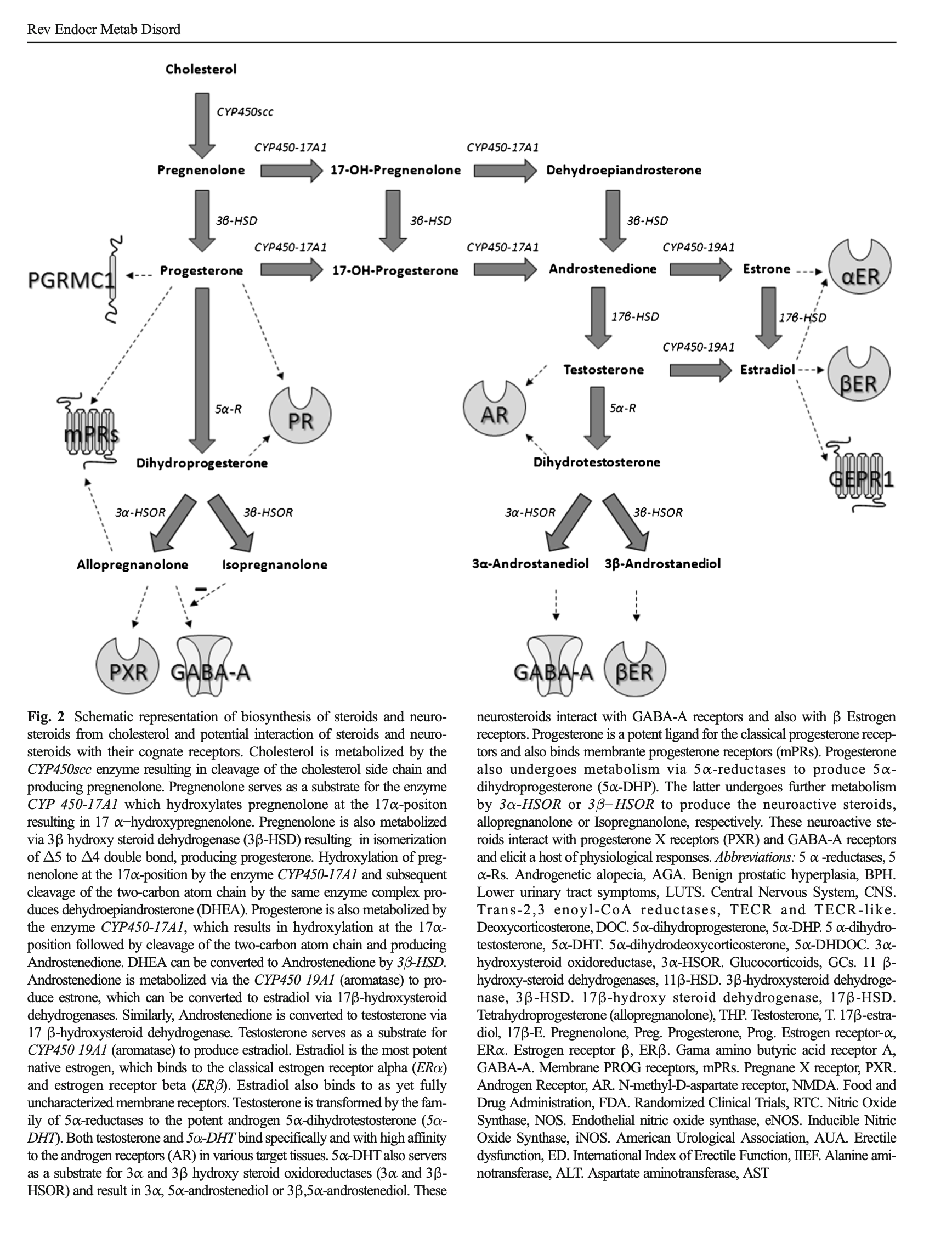
Adverse effects of 5α-reductase inhibitors: What do we know, don’t know, and need to know?
Rev Endocr Metab Disord
Traish AM, Melcangi RC, Bortolato M, Garcia-Segura LM, Zitzmann M
http://doi.org/10.1007/s11154-015-9319-y
https://www.ncbi.nlm.nih.gov/pubmed/26296373/
Attaching pages 1-5 as images (can’t upload PDF). Scihub has the full text. To find it, enter the DOI: 10.1007/s11154-015-9319-y
See especially Sections 1-5.


2 Likes
Unfortunately it does’t show the full article here.
I highly recommend this article to anyone who whats to understand PFS. It also explains really many of the other symptoms like neurological deficiencies, blurred vision, increased risk for diabetes, cancer, heart-disease, stress intolerance. 5ar could even explain pain and skin changes.
I find it highly concerning that blocking 5ar inhibitors lead to death of brain cells! I am highly convinced that future studies will show increased risk for Alzheimer’s and Parkinson’s for Finasteride users.
If you have problems to read the full article https://link.springer.com/article/10.1007%2Fs11154-015-9319-y, some people use sci-hub.se to get around the paywall. Probably legally gray.
2 Likes