Let us look at a couple of things.
- Many men were on fin with few side effects until they crash at a seemingly random time.
- Numerous men have been on fin or dut, quit and had no problems only to go on it once more and crash after an unspecific time.
- When men crash often the crash only takes 12,24,36 hours. They go from feeling fine to being screwed up.
- Once the crash happens the side effects are quite persistent.
How to we explain these undeniable observations? There must be a good reason for this.
I believe the most simple explanation is that fin caused a hormone producing adenoma or hyperplaysia in our body. This can easily fit in with the above four observations.
- You will only feel the direct sides of 5ar inhibition till and adenoma or cell hyperplaysia occurs. This can happen at any time. From day 1 to 10 years or more. Once you do get it you will have a whole set of new sides which you did not feel during your first week or so on fin when you were only experiencing low 5ar.
- Again, you will not have any persistent problems till the hyperplaysia/adenoma develops. You can go on and off fin as many times as you want as long as hyperplaysia or adenoma does not develop.
- Once the adenoma develops your whole hormone balance will fall apart as you are now producing an excess of some hormone or metabolite.
- There is no reliable information on the persistence of adenoma but it is well known to be a long lasting condition which while it persists affects the hormone balance in the body.
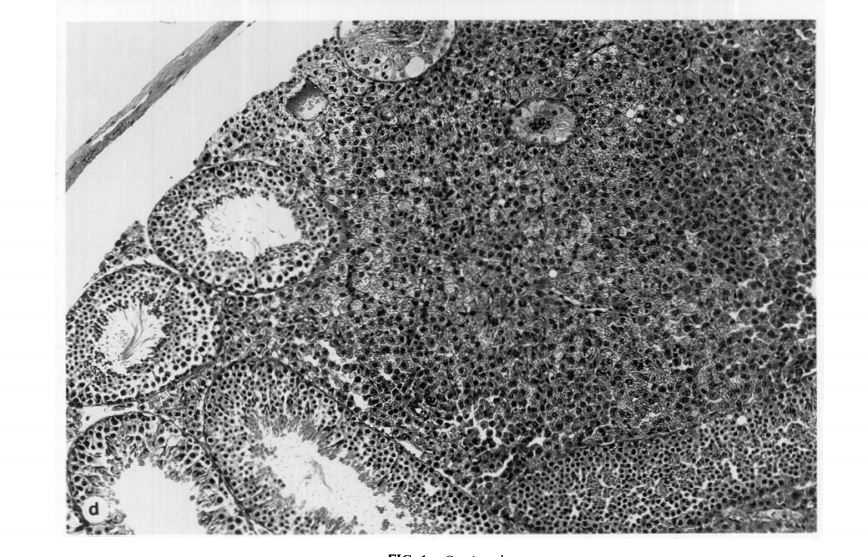
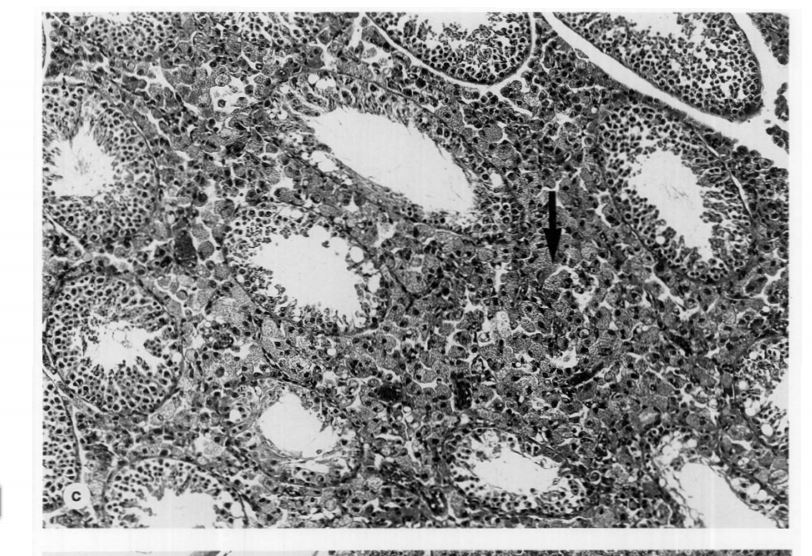
The good news is that PFS has already been demonstrated in mice in 1996. But unfortunately this has not been investigated further. When mice were given fin at a high does for 8 weeks about 16 developed a leydig adenoma in one of the testicles and about 4 in both. The rats obviously did not have the choice to quit when they started experiencing sides as we did and they were taking a much larger dose. Even then only a percentage of the rats got it. With a lower dose of fin less developed hyperplaysia which is a small adenoma. So I guess that in humans at a much lower dose we were the unlucky ones that were affected by this condition. If the dose was increased to say 100mg per day I am sure we would see more men with PFS.
An adenoma can be very small. The size of 3 seminiferous tubules which are less than 1mm. But by definition an adenoma is often described as autonomous, hyper excreting cells. Hyperplaysia is basically an adenoma which is smaller. Of course adenomas can get much larger and it was mentioned some of the mice had much larger adenomas.
I have done extensive hormonal testing and this pattern seems to match what I am experiencing. The difficult part is to work out exactly which hormone or metabolite is being produced in excess. The problem is that there are just so many and a lot of them can not be tested in regular labs.
For myself my urinary hormones are a mess it looks as if the body is trying to dump my hormones out including T.
Obviously once you have an adenoma it is always going to be there and taking TRT or any other hormone is not going to stop it producing excess hormones. Taking external hormones is likely just going to make you feel worse as it is another thing your body has to juggle. I believe our bodies are doing the best they can under the current situation. Many have low free T here including me. There is a good reason for this I am sure.
If you have not read the study about the mice you really should in full. I am not sure I can post it here due to copyright issues. But I can send you a copy.
I have attached some pics of focal hyperplaysia and leydig adneoma in mice.
Maybe some of us can recover over time. For the rest of us, I think we will recover as soon as the offending adenoma / hyperplaysia is removed.