
I think he means stem cells.
who been cured with stim cells?
OK…just spitballing here, and hopefully someone more in the know than me can shed some light, but is the implication of this research that its not actually a receptor problem, rather something is broken in the hormonal pathway? If we have low levels of certain things and higher levels, doesn’t that mean that the regulation/production of these chemicals has been somehow altered? Does this rule out the androgen receptors as being the problem?
These findings perfectly corroborate the over expressed AR hypothesis.
but what can we do about it?
does this also explain why after i stopped propecia my real hairloss started?
Has anyone here tried progesterone with an aromatase inhibitor?
This study doesn’t tell us WHY the hormones are out of whack, but it does tell us that they ARE. Which is HUGE news, since finding a consistent biological indicator of PFS gives us a clue into finding what is actually broken. I really hope neuroscience is at a level where the pathways are well understood, and simple tests can determine why the hormones are not in the appropriate equilibrium. I REALLY hope those tests are already underway…
Yes, I think he uses google translator and means stem cells.
Really though? Cured of what? PFS? Source? No one has been cured of PFS by any treatment, and certainly not by injecting their own adipose derived stem cells back into their blood stream. It doesn’t help making these completely incorrect statements at a time when we’re under the figurative and literal microscope of the research community.
No they don’t. Did Prof Melcangi once mention androgen receptors as being the cause of this?
Now we have this study and rumours of increases AR levels in NUMB genital skin. How do we put it together?
Well, there is zero evidence that upregulated ARs can reduce DHT, 5aR, increase estrogen or inhibit Neurosteroid synthesis.
However, we know that inhibiting 5aR upregulates Androgen Receptors[1] AND reduces DHT, increases estrogen and inhibits neurosteroid synthesis.
Therefore the problem lies with 5aR. Occams razor and all that!
But you said the problem was Phantom DHT antibodies of a neurological basis.
Seriously Oscar, go away. Your Phantom DHT theory didn’t exactly rattle the scientific community. Now yield this forum to those who come to work.
If all 3 subjects were suffering low testosterone it could explain a lot of things, as hormones can alter the levels of neurosteroids. A similar study with subjects with normal hormone levels and still experiencing pfs symptome along with abnormal ones would be interesting.
[quote=“Costa”]
If all 3 subjects were suffering low testosterone it could explain a lot of things, as hormones can alter the levels of neurosteroids. A similar study with subjects with normal hormone levels and still experiencing pfs symptome along with abnormal ones would be interesting.
you have here people with good hormones values and still suffer from pfs.
I know man. I am one of those. That is why i think that people with good hormonal levels along with people with low hormone levels, all with pfs symptoma should be examined. This would rule out the possibility that the neurosteroids are altered due to low hormones rather than pfs itself.
I know it’s been a while, but my current protocol of Progesterone and DIM is similar to Progesterone and an AI, though maybe an AI needs to be used instead.
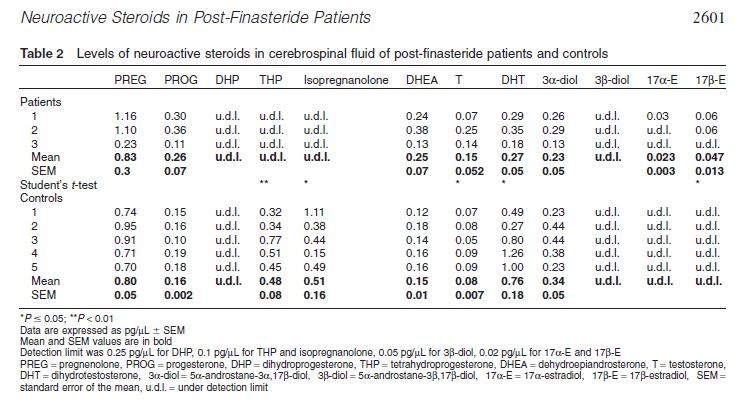
Low 5ar activity in the csf?
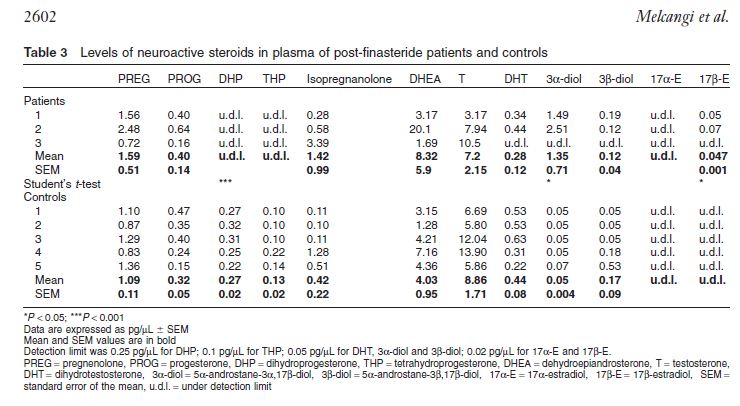
with such a small sample it’s very difficult to understand. basically i was thinking, by looking at the MEAN that in plasma DHT was being excessively converted into something else because there is a much higher than usual value of 3alpha diol, which is a metabolite of some DHT metabolisation into something else (if i udnerstood properly).
but then i realised they are making MEANs with only 3 people…of which subject 2 seems to be an outlayer for DHEA and subject 3 an outlayer for 3alpha diol…
they probably should have taken a few more people on board?
by the way, how do you test the CSF? Is it painful??
One take away I see, and yes I know small sample size so it can’t be generalizable to the entire PFS population, is the CFS levels of Tetraprogesterone and Isoprogesterone in the control group is detectable in the control group and undetectable in the PFS patients, addtionally PFS patients have Estrogen metabolites in their CFS fluid and the control group does not. What does this mean, I’m not sure but all 4 of those markers are made from Progesterone according to steroidgenesis.
Indeed that’s a very good point, and I think we can try to conclude more through that.
Another thing I think it’s concludable is that this PFS thing has different profiles.
That subject number 3 has clearly a different profile from the other 2.
Maybe we should start separating the symptoms and doing a statistical distribution of symptoms vs. blood exams, and try to see if profiles show up…
could we know in that study which were the symptoms of each subject?