
I remember. He got 1g every day infused for totally 5 days. Each Infusion took about 1.5 hrs.
1 g is huge. Mayo thought to be able to treat bis ataxia. With no effect in that.
I wonder why the JPEG is not loading.:)
I’ve been dosing tiny amount of methylprednisolone for one week. At this moment I don’t see any effects.
Tiny dose might not help. He got infused! (more absorbtion) huge dose!
I suggest going on a low dose dexa for one week and withdraw by taking every second day for two weeks.
Yep, I wouldn’t do it w/o medical supervision. Sexual plumbing has worked perfectly for over a year. But who knows whether methyl steroids helped. I didn’t even test the plumbing for several months after treatment. I felt no difference whatsoever “in my head.”
Just boosting this old thread in case you missed it:
It gives me hope to read that you’ve fully recovered in those areas you mentioned, especially the pain and physical impotence. Glad to hear all of that. With that said, could you expand on the methyl steroid treatment the Mayo Clinic gave you? Why did they recommend it, what did it do for you, and do you think all of us should be treated with it?
Probably your posts are the most valuable of propeciahelp. Surely methyl roids reversed the insensitivity of the androgenic receptors and producing 5 alfa reductase.
2 Likes
Thx, just trying to be helpful
COPY FOR AUTO TRANSLATION
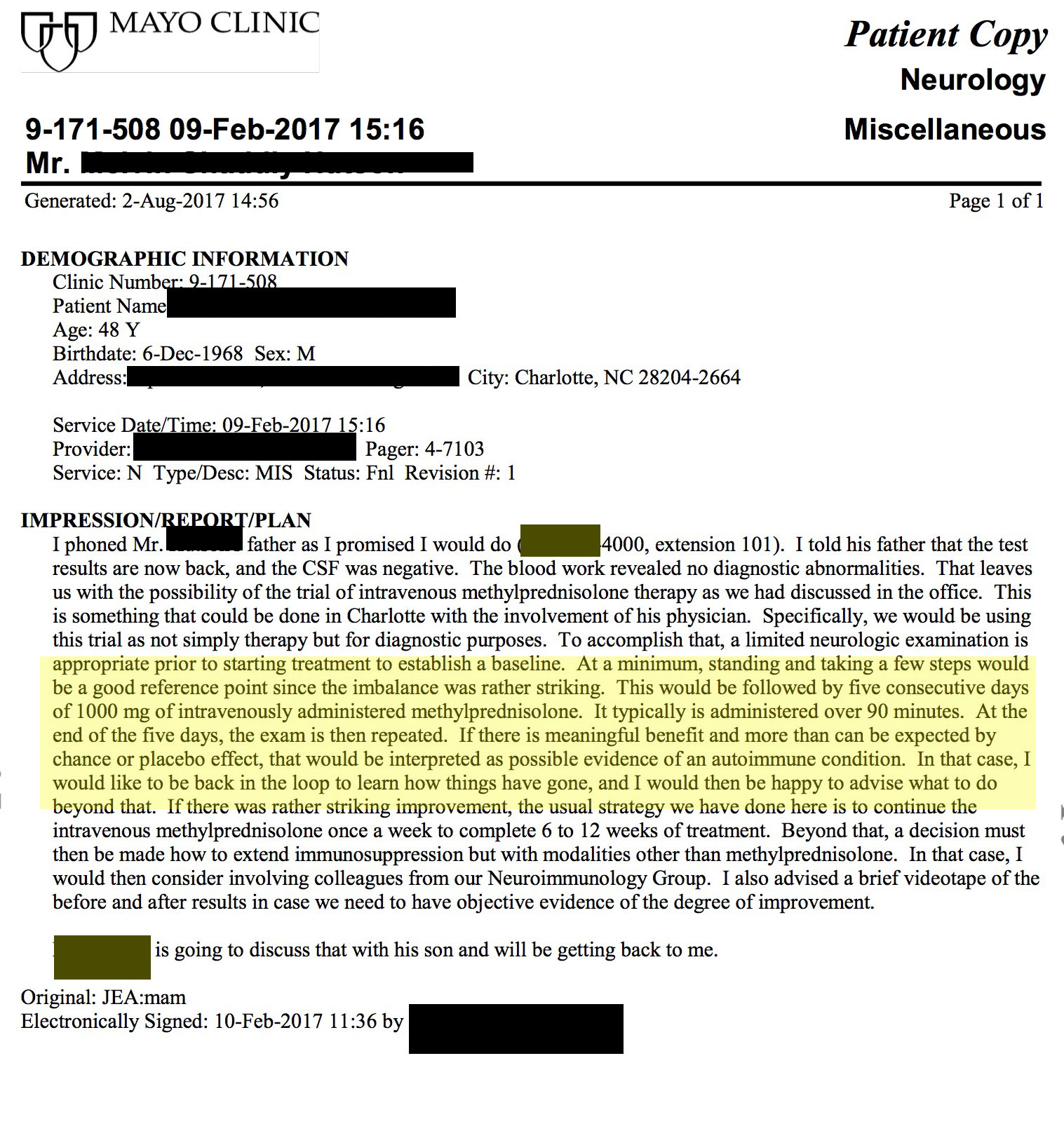
The blood work revealed no diagnostic abnormalities. That leaves us with the possibility of the trial of intravenous methylprednisolone therapy as we had discussed in the office. This is something that could be done in Charlotte with the involvement of his physician. Specifically, we would be using this trial as not simply therapy but for diagnostic purposes. To accomplish that, a limited neurologic examination is appropriate prior to starting treatment to establish a baseline. At a minimum, standing and taking a few steps would be a good reference point since the imbalance was rather striking. This would be followed by five consecutive days of 1000 mg of intravenously administered methylprednisolone. It typically is administered over 90 minutes. At the end of the five days the exam is then repeated. If there is meaningful benefit and more than can be expected by chance or placebo effect, that would be interpreted as possible evidence of an autoinmune condition. In that case, I would like to be back in the loop to learn how things have gone, and I would then be happy to advise what to do beyond that. If there was rather striking improvement, the usual strategy we have done here is to continue the intravenous methylprednisolone once a week to complete 6 to 12 weeks of treatment. Beyond that, a decision must then be made how to extend immunosuppression but with modalities other than methylprednisolone. In that, case, I would then considerar involving colleagues from our Neuroimmunology group. I also advised a brief videotape of the before and after results in case we need to have objetive evidence of the degree of improvement.
1 Like
anonymous1968
have you followed up with your doctors at the Mayo clinic at all? Obviously this is not something we can try on our own
This is incredibly fascinating, are there more than the accounts above that an immuno-suppressant methyl-steroid treatment has rapid effects like this? Could this really be an issue with the immune system?
Couple questions:
How would I talk to my doctor about getting this treatment? Seems like something intense to ask a doctor for PFS issues.
Are there any side-effects to the treatment that should concern me?
Were you taking ANY other supplements or protocols during this time?
This could be a pathway to a cure
4 Likes
Been lurking on this site for a bit. Quick background, I never took fin but I did take steroids for 3 years. The most damaging were deca and tren. I’ve quit them completely but sexually I am completely disfunctional. Most of my symptoms are very similar to PFS. I’ve addressed the low testosterone issue and I feel great in every aspect except sexually.
After reading this, I immediately ordered dexamethasone and I will use it as soon as it gets here. I haven’t been able to have sex for a year and viagra/Cialis/levitra barely work. My main issue is libido I think. But nonetheless, I will try dexamethasone as soon as it gets here. Any suggestions on dose and how long I should use it?
2 Likes
Following up on my questions from above, anyone else have any insight into this? Could this be that when DHT dissapears during FIN use, that a certain virus or even stomach bacteria appears, that prevents the androgens from working once DHT is re-introduced to the body?
This would be about reducing your immune support, so it sounds like maybe the immune system is attacking something when DHT tries to return.
I seem to recall a bunch of people getting cured from certain anti-biotics as well.
Any other theories or puzzle pieces to connect?
2 Likes
A common issue many with PFS seem to have is watery semen, and much less volume of it, with little to zero pleasure. Before your IV treatment with methylpredisolone, did you also experience this issues? And after, were they resolved, or reduce in any way?
2 Likes
Hi @Bicep321, any update on your protocol with dexamethasone? Also, does dexamethasone have similar effects with methylprednisolone, which is what they used at the Mayo Clinic?
I once used oral corticosteroids for a couple of months, way before I took finasteride, and it completely killed my libido. My libido recovered completely after I stopped the pills. I don’t know if that’s relevant.
Has anyone done research what effect corticosteroids have on sexual function and on other hormones such as testosterone, DHT, etc? As I wrote above, corticosteroids killed my libido (and produced depression/anhedonia/apathy) when I took them long before I had started finasteride. So at least that’s some indication that they do have an effect on androgens. Whether it is the right effect is a different question. It is entirely possible that they reduce angrogens which may in fact be beneficial for PFS. Or not.
1 Like
Interesting observation @Sibelio, and the answer is yes. I’m aware of several temporary improvements with dexamethasone. You may be interested in this: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-2265.2009.03683.x
Relative expression of SkM androgen receptor was similar in male (1·63 ± 0·37) vs. female (1·57 ± 0·30) subjects, despite the significant difference in plasma testosterone levels…Following dexamethasone, there was a significant down‐regulation of SkM androgen receptor (1·60 ± 0·23 vs. 1·11 ± 0·16, P < 0·05)
2 Likes
This is quite interesting. Do you know how temporary/permanent the improvements were? If they were just temporary, did PFS return to baseline after a period of time or did the baseline change? If so, I wonder if a longer term treatment with dexamethasone would not elicit a more permanent response as potential epigentic changes make ARs permanently downregulated. Have you considered taking dexamethasone yourself, @axolotl?
After an initial profound improvement it stopped working entirely for the person i spoke to about their experience (xptriado). And no, I don’t consider there to be a basis for expecting that as the driving factors (in terms of genomic loci/expression) are unknown. In terms of myself: No, I don’t believe it’s safe - particularly for severe cases - to mess with things with antiandrogenic properties at this stage of understanding.
1 Like
Sorry don’t have much to add here. I don’t understand medically how “methyl steroids” could effect sexual dysfunction other than the term “steroids.”
I CAN report that my “sexual plumbing” continues to work fine since June 2017. Like PFS never happened.
I do encourage others to try the intravenous procedure I “endured” for five days. See my med note. It could be a total waste of time, could be helpful, who knows? I don’t think it’s dangerous, as it had no effect on me other than possibly ameliorating sexual dysfunction.

5 Likes