
I think you severely overestimate the role of libido. And yes, I am sure we can debate this without reaching an agreement. But that does not mean it is not a debate worth having. So, please provide the evidence that made you 100% certain that all psychological side effects are caused by decreased libido. How do you know it is not the other way around?

I may be one of the few here who has taken both…Accutane as a teenager which stopped my cystic acne and I had blood tests they monitor your liver on Accutane…I stopped treatment early.
Then generic Finasteride in 2014 which didnt do anything but make my hair loss worse fast…
1mg Propecia in 2015 for 6 months gave me horrible symptoms then after stopping the following months I began a journey of health loss like I would have never thought possible…
I could be wrong but the study where they found overexpression of the AR was localized in the skin of the penis and in the BWH study they don’t say where the skin samples were taken from. Maybe it’s different depending on where the skin is taken from? Just thoughts
4 Likes
Very likely @acne1776 - epigenetic changes are site specific. I would expect the results from the coming tissue analysis to be quite different.
The skin in the bwh study was taken from the upper back (I believe in a departure from agreed protocol) and the appendices of the study (accessed separately from the main paper for some reason) suggests there was differences in “a few” androgen dependent genes. It did not specify which. They dismissed this because their correlation method did not pick up on a consistent pattern. The fact this was glossed over in a couple of undetailed sentences was disappointing, as with most aspects of this costly waste of time.
5 Likes
That is of course correct. But given that:
- finasteride is primarily an inhibitor of 5ar2
- 5ar2 is strongly expressed in the genital region (prostate, penis)
- a clear effect in the form of a deregulated AR has already been found in penile tissue
- erectile dysfunction is a commonly observed persistent adverse reaction with PFS patients
- back region has been documented to not be particularly rich in 5ar2
What was the motivation of Bhasin to choose back skin which afaik has not been documented to express high levels of 5ar2 in adults instead of previously validated penile tissue? Why was origin of skin not mentioned anywhere in the main paper (only in a separate appendix)? Why was it not disclosed specifically which androgen-dependent genes were investigated? In the appendix, it was mentioned that “a few” androgen-dependent deregulated genes had been found, but not which ones. Why was this not mentioned in the main paper?
For me, this paper was carefully designed to show that the PFS patients are simply depressed, and to distract from any cell level damage as has been previously found. The only reason I see for such a top notch scientist to produce such a lousy paper, and given the substantial budget he had, is sabotage. Anyhow, I will arrest my case now. This topic is about Accutane.
19 Likes
Something that is overlooked.
Accutane has been shown to be a very potent competitive inhibitor of RoDH4 at therapeutic concentrations of the drug and RoDH4 has been identified as one of the “molecular switches” that governs ligand access to the androgen receptor through conversion of A-diol to DHT, a so called “back door” pathway. There is a nice description of the blocking of these oxidative HSDs as a potential acne treatment in this patent application. Unfortunately, data regarding whether Accutane does or doesn’t competitively inhibit any of the oxidative 3a-HSDs except for RoDH4 appears to be absent.
This back door oxidative pathway may be crucial to maintaining DHT levels by countering reduction of DHT to A-diol.
The direct enzyme inhibition could explain the “early” anti-acne effects (and side effects) of Accutane that are observable after only 1 week and before mRNA levels of steroidogenic enzymes (such as 5ar-I, 3b-HSD, and DHSR9 (an oxidative 3a-HSD)) are significantly decreased, as they are after 8 weeks of treatment.
3 Likes
Dubya! Maybe this explains my condition. After taking the second pill of Accutane, i remember my low back hurting that morning. My lips were dry and my facial skin started to fall apart. This all went away except sexual sides. Do you have any idea why this happened to me? Maybe my prostate was prone to kind of a disease from the beginning of my life… How the hell i get this from 4 pills total. My DHT should have healed itself if it was the real problem.
I think the sharp reduction in DHT causes this problem. It doesn’t matter if DHT production returns. Putting out a fire doesn’t fix a burnt-down house.
2 Likes
Dont think so, because a lot ofmpeople feels better afternquitting, during 2,3,4 weeks, and then crashed.
Somis not dht reduction.
Regards.
Have you ever tried DHT or test?
No, not yet. But i did try creatine and some other supplements, no significant improvement has been seen. Did you use it?
Sorry to bumping up this thread again. But i wanted to ask something about these studies Awor, as we all can see the first two studies are about the lacrimal glands in the eye. And the other ones are about facial skin and AR’s. Are we assuming that Isotretinoin has the same effect on every other tissue and body part because of these stuides?
There aren’t any study done where they examine Isotretinoin’s effect on male genitalia? It is also weird that i didn’t experience any sides besides low semen volume at the beginning. Is there a chance that PAS affects some certain tissues, upbringing underlying problems there, instead of damaging the whole endocrine system and pituitary glands? I wonder what you think Awor. Btw, i still have acne but still have sexual symptoms too.
Im pretty confused. And by the way, if it did damage the AR’s on brain or the genital skin, we should have see everyone suffering from our side effects while on the drug. But they didn’t. I have read that T alone can replace the effects of DHT. So maybe our issue is somehow T can’t replacing the effect of DHT which we could have resolved it with supraphysiological levels of Testesterone which Mohit Khera suggested. (He advised my friend’s doctor to use high dose of HCG for his PAS)
The studies show mechanistic effects on antagonizing/deregulating the AR. It is safe to assume that these mechansims also apply in other parts of the body besides skin, in the same way that finasteride doesn’t just limit its action to the scalp, unfortunately. Here is some more reading btw:
2 Likes
I think it’s interesting that my hair loss and receding stopped despite heavy steroid use. I receded 3cm and it pretty much stopped there. I was using accutane in low dosages along with steroids for years… Around 6 to 7 years daily. I wonder if accutane stopped the hair loss. The stuff I use would make someone prone to MPB very bald very fast. For example masteron is a DHT derivative known for hair loss in those prone to it.
What does that mean though? Androgen receptors are not functioning correctly? I also seem to need ridiculous dosages of testosterone just to feel normal and I aromatise very heavily into estrogen. More than 99% of people.
I think there should be retinoid receptors on that particular tissue for Accutane to cause damage? No? Are there retionoid receptors on genital skin?
In the study it says, they took biopsies from back skin. And they lost %80 of ability to form DHT and they had reduced AR binding capacity…
If this applied to all of the other parts, including genital skin. Doesn’t everyone should experiencing PAS and PFS?
I don’t think this applies to whole of the body, otherwise it does not make any sense. Everyone should have experience sexual sides on this drug. I took Tane only for 3 days and my skin started to peel off for a week after i quit!! But went back to its oily state after. If it wasn’t tissue spesific i should have seen a reduction on my acne, which i didn’t.
@Dubya_B Do you think these inhibitions return back to normal baseline after quitting the drug? On normal people it should, otherwise they should experience sides like us right?
You are true.
When studying the (side) effects of isotretinoin, there are many similarities between at first glance very different effects. One cause of this is gene expression. A gene that is expressed in the skin may also be widely expressed in cells of the brain, liver, kidney, heart, and many other cells. This is the case of the retinoid X receptor, RXR, which is strongly affected by the retinoid 13-cis-retinoic acid (Roaccutane). This means that when the substance is used in very high doses, all the cells that carry these receptors will be affected. As an example, let’s examine this retinoid receptor by consulting a gene database.
Genecards - RXRA (Retinoid X Receptor Alpha)
https://www.genecards.org/cgi-bin/carddisp.pl?gene=RXRA
RXR comes in three forms. We’ll take a look at RXRalpha (RXRA).
And again, as if by chance, we see that its expression is not confined to the sebaceous glands… Quite the contrary…
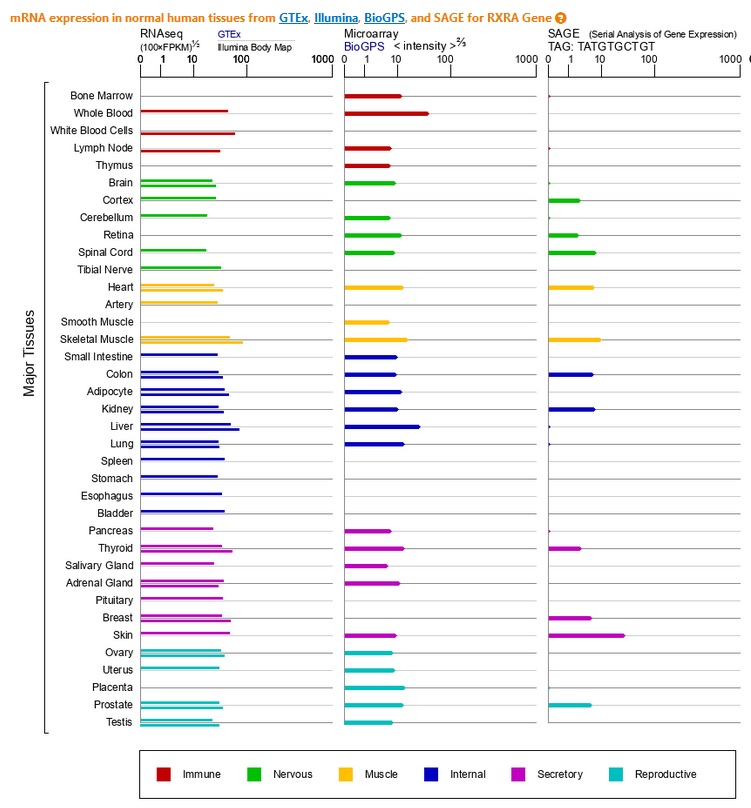
It is expressed everywhere: Hormonal, reproductive, intestinal, immune, musculoskeletal, nervous systems…
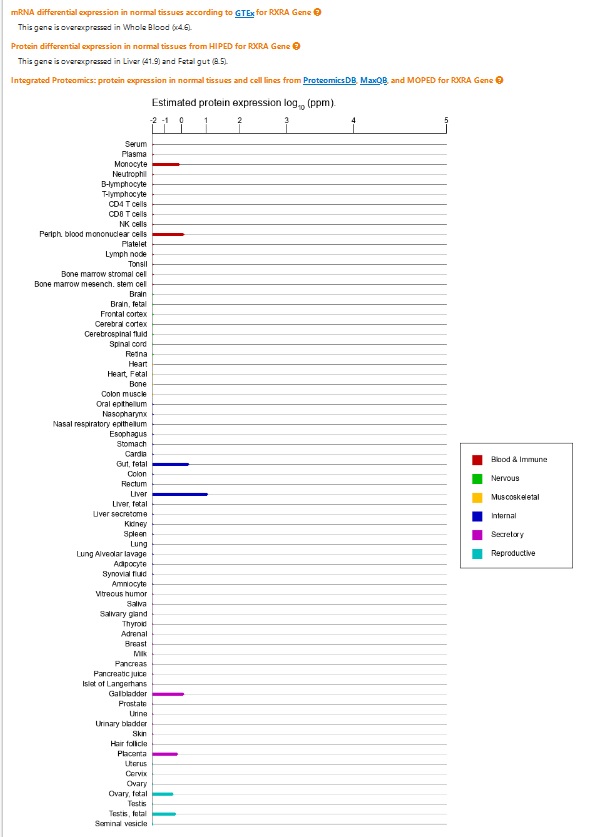
This gene is overexpressed in whole blood, in the liver, intestine, immune system, gallbladder, placenta, reproductive glands, etc.
1 Like
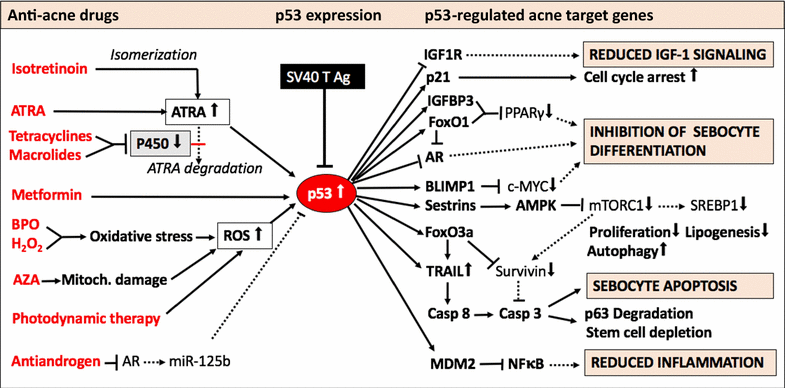
There are cascade events happening which end up with p53 overexpression —> consequent foxo1 upregulation which in turn downregulate/block AR and reduce sensitivity to androgens. There is enough literature on it.
RXRA -> p53->foxo1-> AR
Friend, excuse my English, but in this case what would be the line of treatment for dna demethylation? I don’t understand much about
Friend, excuse my English, but in this case what would be the line of treatment, DNA demethylation? I don’t understand much about