First, sorry to hear you’re not feeling any better. It’s tough, but keep fighting. Years down the line, guys have shown improvement. You never know what is around the corner for you.
Second, I think I’m right in saying that these results are pretty big news. Thanks very much indeed for bringing them to the forum.
Only you and Awor have managed to have these kinds of tests done. It’s really important that you talk to Awor about what you’ve discovered: as he mentions above he is planning further testing with a scientist he’s working with, and these results may help them plan that.
AR binding and dissociation rates were normal. This is in line with what Awor discovered when his scientist tested binding. It seems that the post-finasteride syndrome is not about dysfunctional binding and dissociation rates.
AR gene mutation and deletion were negative. I know that Awor and his team are planning to look at gene expression of the androgen receptor. I don’t know if the test that you have had is the same as the test they want to run. It sounded to me as though Awor’s planned test would be extremely expensive and take many months.
But I don’t know enough about it all. That’s why you definitely should get in touch with Awor, and talk to him and probably to his scientist about the nature of these tests and the results.
These results take us a step forward in learning the true nature of our condition: great work.
As mentioned previously, there can be defects in AR function even with NORMAL binding and dissociation. More investigation is required.
Human minimal androgen insensitivity with normal dihydrotestosterone-binding capacity in cultured genital skin fibroblasts: evidence for an androgen-selective qualitative abnormality of the receptor. pubmedcentral.nih.gov/articl … id=1684524
www3.interscience.wiley.com/jour … 6/abstract
“Appreciable unexplained interexperimental variation of the DHT-binding activities in genital skin fibroblast strains demands that multiple assays be performed on a strain before its receptor status is classified quantitatively. In our experience to date with genital skin fibroblasts, four of 13 propositi with CAI have been receptor-positive.”
See the below screenshot. DNA binding investigation is probably next step.
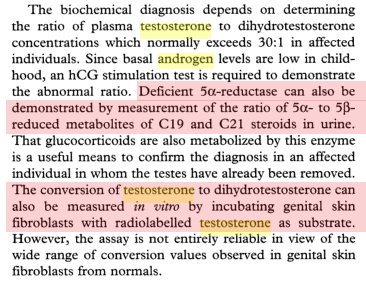
Did you get 5AR2 activity assessed in the genital skin fibroblast culture? That also needs to be assessed, to see wether DHT is converting correctly locally in those tissues post-Finasteride.
What did your doctor say about the results? You should consider further testing per the attached screenshot.
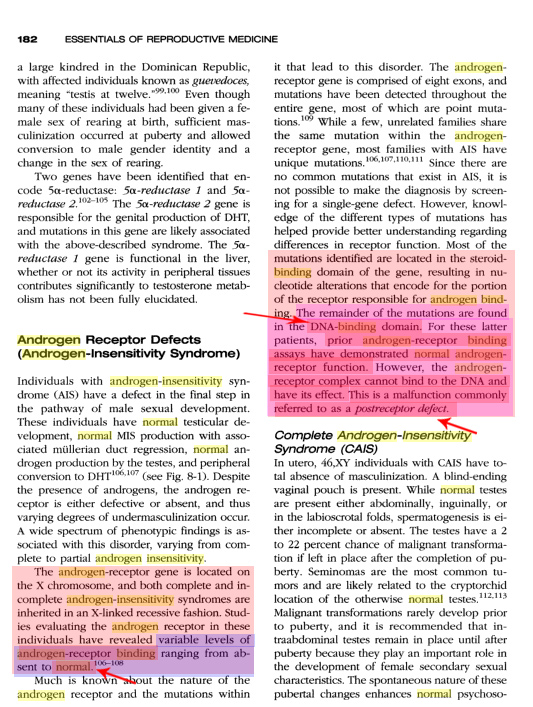
Interesting stuff in that screenshot about “post receptor defects”.
If I understand it right, the textbook says that this is a mutation in the DNA binding domain of the androgen receptor gene. This mutation means than even though there is normal binding, the androgen receptor cannot exert its effect.
We seem to be seeing normal binding without androgenic effect, so this could be what is happening to us.
Only thing is, Chams said he tested the entire sequence of the androgen receptor gene, and found it was normal. Wouldn’t this include the DNA binding domain?
If not, then we need to test the DNA binding domain of the gene to see if there are changes. Presumably this is possible via the same kind of test that Chams had to analyse the rest of his AR gene. Maybe the lab at Addenbrookes could do it. In which case, I’ll go and give them some of my blood.
It feels as though we are getting somewhere. What we need is a scientist who can answer our questions:
Did Cham’s test include the DNA binding domain?
If not, can we test for mutations of the DNA binding domain?
In the light of Cham’s tests, what else should we be testing for?
Awor is working with such a scientist; the only scientist I’ve heard of who is taking an interest in our condition at this level. They’re interested in investigating epigenetic change of the AR. But we need to take these results to Awor’s scientist and have a discussion. I mean, it’s clear this scientist is interested in this stuff: he’s working closely with Awor. It may be that we are a few blood tests away from serious answers.
i m loosing pieces…so what list/kind of genetic test should a guy have to understand the all situation we need?..if someone can write the list,it ll be easier to someone who need to have them done .
thanks Mew and SM for your replies:
my tests were done on the entire coding region, so i don’t clearly get what MEW posted…but anyways,you can always find lots of possibilities,but the question is about the availability of tests to include or exclude what you suggest.
my Doctor didn’t know about epigenetic changes. i couldn’t find even one lab to do a test for epigenetic changes. i don’t know how you guys came up with that test? i don’t know where Awor is gonna make such test.
MEW if you suggest other tests please name them…5AR can be availabe,and that will be my next step. i have discussed with the doctor if it is possible to take a prostate biopsy and test it ,and i think it is possible.
will keep you guys updated.
Why is that? DNA binding is just another intermediary step in the chain. You just as well can start looking at various known (and unknown!) co-activators and modifiers (which could just as well be the problem*). In other words, this test can turn out normal and you still don’t know what the heck is going on. Just like the receptor testing chams and I had done. We now know that his receptors work and that mine work. Great, but that doesn’t advance us an inch. We can drill another hole into the pipe (=DNA binding) and peek in. Maybe we’ll see something, maybe we won’t. Or we can go to the end of the pipe and look through (=gene expression) and see what’s in there - once and for all. What makes more sense to you?
Guys, let’s get a little focused! We’ve got clear advice from a scientist so far telling us the next step is to test actual gene expression. Gene expression is the end of the chain. In other words, if gene expression turns out normal, then there is no point in looking at anything else “upstream”. If the test turns out negative, then we know that the problem lies somewhere in the nuclear processes downstream. A scientist needs to tell us what to look at after that.
Look mew, it took a lot of effort to find this scientist and get to the information level WE now have. You know that. And you even participated in this effort. Why don’t we just believe what this androgen receptor specialist/scientist says and not try to out-google and out-smart him.
Unfortunately, the lab this scientist works in doesn’t have the (rare) equipment required to test gene expression. Otherwise I would have had the test done and shelled out the cash it takes to do it. We now need to find a lab to perform this gene expression micro array test. It will be expensive but we can get together and pitch in. Perhaps chams can check if his lab has the resources to test this. I will continue searching on my side as well. I’ll keep you guys posted. I am convinced that we will eventually get there if we stay focused.
this statement also originates from the scientist in question
sorry MEW,i didn’t reply to your questions:
first off: my doctor never believed that i have androgen insensitivity syndrome. he said it is congenital defect and there is no evidence whatsoever that finasteride could cause this. he ordered those tests for me because i kept asking for them, and because he has run out of ideas, so to speak.
5AR test will be my next step, i haven’t done it yet.
i have a question for you Mew,or anyone else here: do you have any idea about the mechanism of androgen uptake by human cells? androgen receptors are inside the cells,so androgens have to be uptaken first by the cell in order to bind to receptors. do you have any studies about factors that may affect such uptake process?
it is true that androgen insensitivity syndrome is a congenital defect. but there are many other reasons why a ligand (hormone) binding to a receptor doesn’t exert the normal/desired effect (=gene expression). The receptor is only the TRIGGER to a series of very complex processes which follow. To take a car analogy: Our receptor tests only tell us that the key fits into the ignition switch. We can now turn the key but nothing happens. It could be a fuse, the battery, no fuel, the starter or a number of other things. All those things need to work correctly for your engine to start. The only difference with a car is that you can open the hood and physically see the engine running. We obviously can’t do that at the molecular level. So the running engine would be the equivalent to gene expression in our bodes. The gene expression test would tell us if turning the key (hormone binding to receptor) actually does anything at the “engine level”. And THAT is what we need to find out.
My doctor firmly believes that our problem is “downstream” from the receptor. He believes that fin CAN cause epigenetic changes which can explain this. Separate from this, I have the statement of a scientist that did the functional receptor tests that we need to look at gene expression.
Yes, agreed this would be the ultimate way to check wether things are working correctly or not – perhaps I am a little uninformed in terms of the “chain of events” and thus thought DNA binding was more towards the “end of the pipe” than it really is.
Awor, can you clarify all the steps involved? From a high-level standpoint, my guess is something like this, although I’m sure I’m missing many steps:
Androgen Receptor --> 2. AR receptor binding complex --> 3. DNA binding, ligand mRNA binding? --> 4. Gene/protein expression
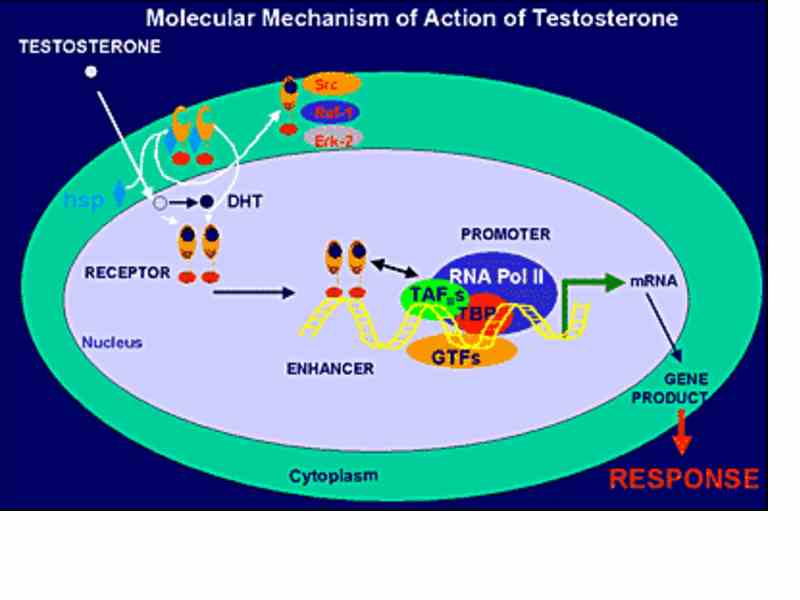
andrologysociety.com/resourc … 11fig1.jpg
“FIG. 1. Mechanism of androgen action. Testosterone (T) enters the cell and is converted by 5 alpha reductase to 5alpha-dihydrotestosterone (DHT). DHT binds to the androgen receptor (AR) leading to a conformational change in the protein and the dissociation of several accessory proteins, including heatshock proteins (HSP). Binding of the AR to the androgen response element (ARE), along with other transcription factors (TF) regulates the transcription of mRNAs.”
Agreed. We would need to find someone or somewhere to conduct such tests, a molecular geneticist to provide us the answers we seek. I guess I’m saying nothing new here.
I’m not trying to “out google” or “out smart” your contact, far from it. Like I said earlier, I wasn’t clear on the all the steps involved in the complete AR --> gene expression pathway, so if your contact says Gene Expression is the end of the line, great – we know where we need to look now.
Agreed, that is indeed the next step:
Finding a lab or university research facility that can do a gene expression micro array test
Finding out the costs involved
Finding a research scientist willing to undertake the tests
Now, we all need to individually do our research for facilities, conduct phone calls and emails to find out this information, and keep each other updated as to progress.
Thanks for the update Awor, it is much appreciated. With this knowledge at least we have clarity as to another area to investigate. Wether it will turn up anything of value is still to be determined.
I for one agree with what Awor said, we must get together in this matter,
we need to get to the bottom of this. We are very close in finding the
root cause of our problem.
Since gene expression micro array test is very expensive, perhaps
we should help Awor.
Mew are you willing to organise a fund, it should be on volunteer basis. I can donate 50 US$ a month. Everyone who feel that this cause is important can joined in.
Others who disagreed can simply choose not to donate. It is that simple.
OK, we have from Awor the definitive statement on what we need to do next. It seems we can forget about a DNA binding domain test, and simply go for the gene expression micro array test.
We are one test away from serious answers. If the test is negative, that will rule out a whole sphere of possibilities and still be a significant result.
Now we just have to work to make this test happen.
I’ll investigate the situation over here in the UK.
When we know how much it is going to cost, we can devise a plan to pay for it. Obviously it’s going to need a few of us to chip in.
Awor is right, we need to focus our efforts on this single aim.
Let’s think, also, about the best way to make approaches. Once we have found potential laboratories, is it best if we hand these details to Awor’s scientist, who will call the lab himself to discuss? Most of these labs will not be used to dealing with patients; they are facilities for research scientists and consultant doctors. So it would seem more sensible if the call came from the scientist: he would also know what exactly to ask them in terms of their ability to run the test, the timescale, the equipment, etc.
This is my understanding of how it works based on what I could gather from reading and listening to the specialists:
Testosterone enters into the androgen target cell.
Binding occurs to the androgen receptor either directly or after its conversion to DHT.
Binding to the receptor is followed by dissociation of heat shock proteins in the cytoplasm.
The receptor enters the nucleus via an intrinsic nuclear localization signal.
The next step is the recruitment of coactivators, which can form the communication bridge between receptor and several components of the transcription machinery. Upon binding in the nucleus to specific DNA-sequences, the receptor dimerizes with a second molecule and the homodimer entity recruits further additional proteins (e.g. coactivators, general transcription factors, RNA-polymeraseII)
This communication triggers subsequently mRNA synthesis and consequently protein synthesis, which finally results in an androgen response.
In addition, a non-genomic pathway involving the classical androgen receptor via cross-talk with the Src/Raf-1/Erk-2 pathway is also known.
Mew, you were talking about one of many elements of level 5 and I was talking about level 6. After testing Level 1 (hormones) and Level 2 (receptor binding/disassociation) without result, the recommendation of the scientist is to go directly to level 6 and not worry about the dozens of (partially unknown) factors between level 2 and 6. We can tackle those later once we know if the basic response is here or not.
This is a “simplified model of our current understanding of androgen action in an androgen target cell”. Translated into plain English: Science basically doesn’t fully understand what is going on at the molecular level inside the cell beyond (i.e. downstream from) the receptor.
My purpose in writing this post is to create awareness for the huge complexity of the whole (androgen) receptor function. Combine that with epigenetics - self modification of downstream system sensitivity through currently unknown mechanisms - we (mankind) have only very recently begun to understand that the “other” 90% of our genetic information, which science previously called “junk dna”, actually has a purpose, that is to pass on “learned” information from one cell generation to the next (= epigenetics).
The bottom line is that there are so many things at the sub-cellular level that we just don’t know about. This stuff is simply beyond even bleeding edge science. That is why nobody has figured out yet why Finasteride (and possibly SP) can cause such problems. And if a doctor tells you that it is impossible for Finasteride to cause the Androgen Receptor to fail in this way, he or she is just ignorant. Only a good doctor knows and will admit that we/science do not know everything. That’s the litmus test for your doctor.
Also, just to not get everyones hopes up: I am convinced, we can test it and we will test it (gene expression). We “just” need to get the right setup lab/scientist. I said this before: That will only give us the proof of what the problem is, not the solution. If receptor desensitization (in whatever form) turns out to be the actual problem, we in theory would need to find a way to influence or change the epigenetics involved. The most realistic proposition here is to just give the body the time it needs to repair itself (which we know can take years). Theoretically, supplementing a substance could speed up the process. We have some anecdotal evidence in this forum about various substances that may have helped (Magnesium, Zinc, HMB, Antibiotics*, etc.). In theory, the epigenetic information (which possibly got screwed up) could directly be manipulated. This does not seem to be a realistic proposition though, given the current state of technology.
It is interesting to note that antibiotics work by acting on virulence gene transcription. This mode of action could possibly explain why a number of members have experienced some form of relief or even short recovery while using antibiotics.
Awor, have you talked with your scientist if it is possible to reverse epigenetic changes if we test positive?
Do you know any doctor who is specialized in that field of epigenetics?
I reworded the last paragraph of my last post because it was misleading. Epigenetics is a cutting edge research subject, not something doctors usually directly deal with.
To give an anwser to your question, we would need to know precisely what the problem is. This is not the case. All we have is a hypothesis and a recommendation on what the next step is to prove it. From that point on, it’s a deep dive into basic and very expensive research. Following citation from the above link gives a good overview of the order of magnitude we are talking about:
The following reading gives a short (but very complicated) overview of the currently available technologies for epigenetic manipulation of gene expression: jcb.rupress.org/cgi/reprint/169/6/847.pdf
Following quote from this article tells us that routine application of this technology in humans is still far away.
The hard fact currently is, that the solution to our problem is probably beyond reach. The best we can do at this time is to try out and find simple things that help us get better. Be it some supplement, living healthy or just getting enough sleep. And sharing our experiences in this forum.
Isn’t it weird how this is by the far the most significant thread in this entire forum, but only like five guys are interested enough in it to contribute to the discussion.
hi my friends,i ve found here in italy a clinic testing 5AR 2 gene SRD5A2 by blood… so in few weeks i ll be there doing it … i didn t exactly understand what more genetic test i could do,so please MEW or someone could tell me the name of what genetic test i ve to look for cause i ve found many clinics that have a lot of tests that can be done.

{kind=link}
{kind=link}
{kind=link}