Has anyone done any adrenal testing? Decreased libido may be related to adrenal fatigue. The main cause of adrenal fatigue is stress… While I cannot say what your cause is specifically I have seen patients have improved libido with adrenal support. Caution: adrenal testing and support should be facilitated by a licensed physician.
Hi Dr. Wheeler
I am unsure why you posted this in the Adiol-G testing section, but yes many of us have had adrenal testing.
If you are joining the board, do you care to give us a bit of history about yourself or your practice - as a doctor?
Thanks
I changed subject of his post to “Adrenal Testing”.
He is a naturopathic doctor from Bellevue, Washington, USA.
Hi Dr. Wheeler
Thank you for your interest in PFS and joining us in this discussion. Obviously you have put some thought into the causes of PFS. Other than adrenal fatigue do you have any other insights into our condition? Do you feel this is a treatable condition? I believe alot of us would greatly value a naturopathic viewpoint particularly as we have been victimized by pharmaceuiticals.
Yes, I am a naturopathic doctor in Bellevue, WA. You can visit my website at http://VueWellness.com. I graduated from the National College of Natural Medicine last year and also have a BS and BA in biology and international studies in biology, respectively. I am currently working with Dr. Jonathan Wright, MD and am studying hormone testing and healthy aging medicine, mainly. As a recent graduate I cannot say I have considerable experience working with those effected by finasteride but have talked with Dr. Wright extensively about this drug and his observations.
We do thousands of hormone tests at our lab (http://MeridianValleyLab.com) and specialize in providing the most comprehensive testing possible. While we test for basic hormones such as cortisol, testosterone, progesterone, and estrogens, we also test for all their metabolites and how they are converted in the body. For example. DHEA is converted to Androstenedione, which is converted to Testosterone and then DHT (alpha and beta). DHT is converted to androstanediol (see chart: http://meridianvalleylab.com/hormone-testing/24-hour-urine-hormone-tests/). While this information is very clinically useful and relevant it can be very challenging to interpret so that is why we have several doctors on staff to help other clinicians. We have a long list of doctors who know how to do this testing and can help you find a doctor in your area.
My personal perspective: the problem with finasteride is that it totally shut down your production of DHT and all its metabolites. While too much DHT can cause problems it is really the ratio of DHT to androstanediol that may be the most important for prostate cancer risk (theoretical but there’s lots of research). Interestingly enough even herbs like saw palmetto can be too potent of 5AR inhibitors and we often try GLA or zinc first and then do follow-up testing.
As a holistic doctor I want to get the big picture and the details. I want to see how hormones are being converted for both safety and efficacy. While finasteride may have caused many side-effects, how it caused those side-effects may be different for each person so getting as much information is critical, in my opinion.
What sort of adrenal testing have you had? Salivary, blood, and urine are the main samples used for this sort of testing and each have their benefits and disadvantages.
I hope I can be of help.
Cheers,
Barry
Thanks for the informative response. Regarding my testing personally I have tested dheas and it above range high. Adiol g is below range low.
Hi Dr. Wheeler, thanks for your reply. May I ask:
- What got you interested in this forum and the issue of persistent Finasteride side effects (sexual, mental, physical)?
- How did you come across the Propeciahelp website?
Can you share Dr. Wright’s observations/thoughts as to how Finasteride can cause persistent side effects, and through what mechanisms of action?
Yes, your lab and Rhein Labs (rheinlabs.com/hp.html) appear to offer similar 24-hr urine profiles for both hormones and their metabolites. As you note, it is important to look at the big picture beyond standard hormonal assays. Unfortunately, many in the medical community do not do such hormone profiling when trying to determine hormonal aspects for persistent Finasteride side effects. So, thanks for your insight.
Thanks for your perspective as to one potential cause for our longterm issues, although it is directed at prostate cancer risk (an area of concern, although for many men likely secondary to the ongoing hormonal/sexual/mental/physical dysfunction issues Finasteride has left us with).
As you may or may not be aware, one of the hallmarks of the Post-Finasteride Syndrome is a post-drug drop in Testosterone metabolism, LH & FSH values to near or actual hypogonadal levels within weeks of stopping the medication, after 5AR/DHT is no longer inhibited (ie, did DHT surge back to baseline or beyond baseline after stopping Finasteride? Did this cause negative feedback on the hypothalamus-pituitary axis, causing the drop in Testosterone production? Why would this condition persist longterm?).
Those who have been diagnosed, have often been diagnosed with tertiary/central hypogonadism – hypothalamic (hypothalamus no longer sending GnRH to pituitary. Pituitary remains responsive to clomiphene citrate, LRH and hCG stimulation tests (results show increased LH/FSH response)). Unfortunately, the hypogonadism remains variably resistant to treatment.
Please review the following regarding this very serious issue, and other doctors’ thoughts such as Dr. Alan Jacobs, Neuroendocrinologist’s on the potential causes:
Dr. Jacobs’ posts on persistent Finasteride side effects:
blog.alanjacobsmd.com/alan-jacob … n-men.html
blog.alanjacobsmd.com/alan-jacob … erone.html
Dr. Jacobs’ proposed mechanism (possibility of acquired partial androgen resistance)
blog.alanjacobsmd.com/alan-jacob … eride.html
Dr. John Crisler outlines the issue of persistent side effects, noting that even in men who quit the drug and retain nomal testosterone values, they still suffer from all the symptoms of hypogonadism: youtube.com/watch?v=BEGCTMtlgoc
Many people have theories as to the reason for persistent Finasteride side effects. Based on the above, some have speculated a root cause for our ongoing issues may be due to a drug-induced, novel and acquired form of partial androgen resistance or 5AR2 deficiency… due to loss of DHT while on the medication, causing alteration in androgen receptor/5AR2 enzyme function/gene expression changes or downregulation that persists longterm, due to epigenetic changes.
Of course, none of this has been proven and is simply speculation at the moment. Until we are evaulated in a research lab, we will be no closer to answers.
Dr. Wheeler, as you have likely already read, many ex-Finasteride users with persistent side effects have been found to have below range 3a-Diol-G (3alpha-androstanediol glucuronide) values: viewtopic.php?f=4&t=2763
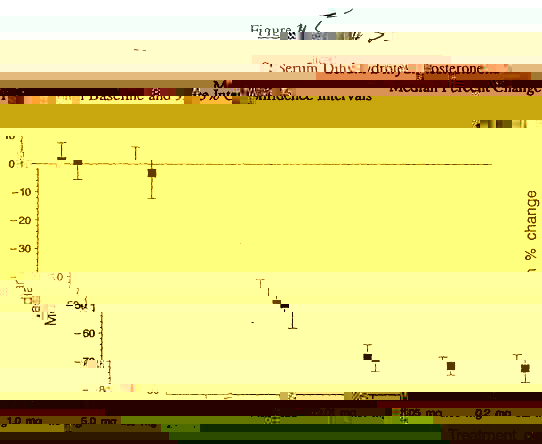
As you are also likely aware, 3a-diol G is a metabolite of DHT involving the oxireductive 3a-HSD pathway. As you can see in the attached screenshots, 3a-diolG:
- is documented to be decreased concomitantly by Finasteride treatment (images from FDA Propecia Clinical Trials)
- is a marker of both 5AR2 enzyme activity and androgen metabolism disorders (low levels of which correspond with androgen resistance and 5AR2 deficiency syndromes)
Knowing the above doctors’ thoughts, and based on these ex-Finasteride users’ below-range 3a-diol G values after using and quitting the drug, can you provide any insights into what these 3a-Diol G results might mean in the context of persistent side effects? Could a dysfunctional 3a-HSD pathway also be involved (and more importantly, how to correct it)?
The truth is, men suffering from this problem have not been investigated in a research laboratory, the medical community at large remain unaware of this potential outcome from 5AR inhibitor usage, and nobody has any real answers as to the root cause of our issues and why they persist after quitting Finasteride.
Personally, I believe our negative response to the medication has a genetic basis, considering scientists are now recommending men be genotyped for 5AR2 enzyme variants when designing 5AR inhibitor treatment protocols ( hairdx.com
Since Finasteride is also documented to affect other pathways such as Nitric Oxide Synthase production (mediated via DHT), the 5AR-reduction of Progesterone to Allopregnanolone and Deoxycorticosterone to THDOC – both vital neurosteroids which normally act on GABA-A receptors in the brain to exert anti-depressant and anti-anxiety effects – it is possible there are other as of yet unknown areas the drug could have altered without our knowledge that are playing a role in this problem.
Thanks for your time and interest in this issue, any thoughts or insights are appreciated.
Mew
Administrator,